You need to know some neuroanatomy to understand how the brain and spinal reflexes affect the muscles. If you want to look at or revise the descending neural tracts from the brain to the spinal cord please see Additional Information for more details.
Here are the normal spinal reflexes and how a muscle contraction works. Imagine you strike the patella tendon at the knee with a tendon hammer.
Reflexes after stroke
Video transcript
Reflexes after stroke
M. So I’m just going to do a little test on the sole of your foot Allan. Just to tell us a little bit about the reflex activity in your muscles since you had your stroke and we can just do a comparison between the two sides. So I’m just going to run my thumb up the foot here. We can see that as I do that the toes just move down slightly. That’s called a flexor response or a negative Babinski. A big name that one. We can compare on this side if we come up this side and we see the toes move up in to extension and that’s called a positive Babinski. So it just tells us that the control of the reflex activity in this right side is affected.
A. Right
M. We can also just have a little look at the reflex activity in your tendon jerk. So if I just rest your left leg here on my hand. Just let your head relax, let everything go. If I just go here we can have a look at your tendon activity here. Just let it go. So very mild, that’s fine. Then we can make a comparison. Again nice and relaxed. We can see the difference between the reflexes of the two sides of your body. We can do this. Test these reflexes in different positions but it is quite helpful in this position.
Bilateral system (influence on the same side as the lesion and also crosses to opposite side)
Has medial and lateral tracts
Involved mainly in postural control. Has an influence on upper limb recovery
Mainly innervates proximal and axial areas – sends information to trunk, shoulder girlde and pelvis girdle muscles, but also to the opposite arm and hand (Baker 2011)
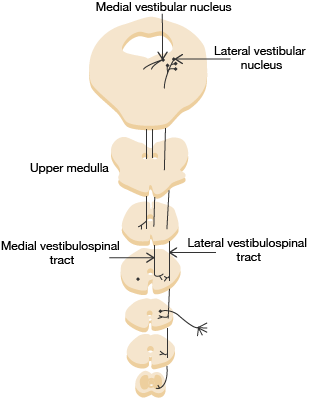
Vestibular system
Anti-gravity activity- (works when we are moving in more upright postures)
Proximal and axial termination (send information mainly to trunk, shoulder and pelvic muscles)
Ipsilateral – same side as the lesion
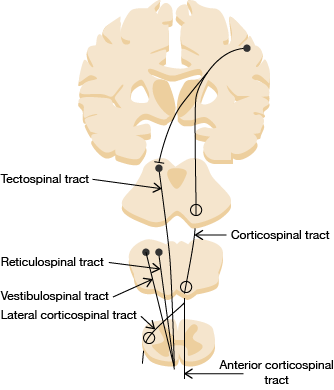
Tectospinal system
Originate in the mid-brain (superior colliculus and interstitial nucleus of Cajal)
Descend ipsilaterally
Responsible for reflex movement of head and neck in response to visual stimuli. e.g. gaze stabilisation on objects during reach
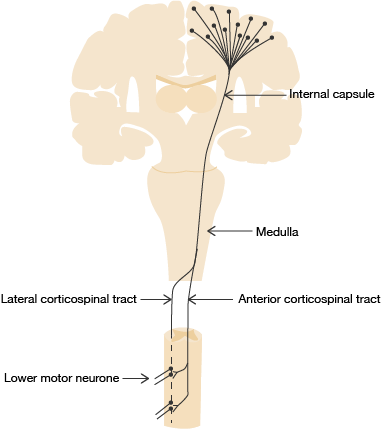
Corticospinal system
Draws fibres from various areas of cortex
Travels via the posterior limb internal capsule, (common site of MCA territory stroke), and through medullary pyramids
90% fibres cross/ decussate in medulla – contralateral
Lateral Corticospinal Tract
10% of fibers remain ipsilateral
Ventral Corticospinal Tract
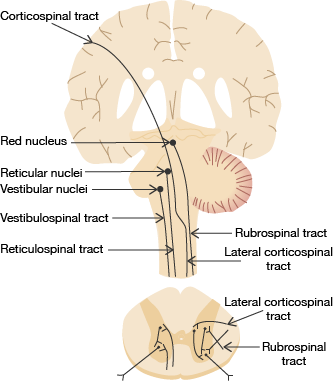
Rubrospinal system
Red Nucleus Humans– magnocellular – small — parvicellular – expanded
Projects to upper limb and, via propriospinal networks, to lower limb
Connections to cerebellum, inferior olive and reticular system
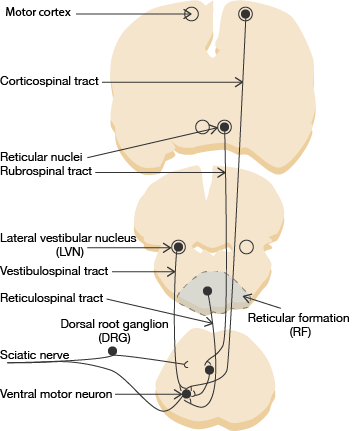
Systems controlling spinal reflexes
Inhibitory – lateral reticular system
Excitiatory – medial reticular system, vestibular system
Corticoreticular pathway – Cortical excitation of the dorsal (lateral) reticulospinal pathwayOther relevant descending systems: Rubrospinal and coerulospinal tracts
Mechanisms involved in spinal reflex activity
Excitability of the stretch reflex circuit (afferent fibers, spinal motor neurons, and efferent fibers) is predominantly regulated by excitatory and inhibitory descending signals of supraspinal origins. In a neurologically intact person, the descending reticulospinal tract (RST) and vestibulospinal tract (VST) provide a balanced excitatory and inhibitory descending regulation.Other descending pathways are either not related to the spinal stretch reflex (corticospinal and tectospinal) or absent in humans (rubrospinal tract) Sheng 2017
Spasticity
Experimental evidence supports the theory of supraspinal origins of spasticity, likely from an imbalance between descending inhibitory and excitatory regulation of spinal stretch reflexes, secondary to cortical disinhibition after stroke. (Sheng, Fransisco 2015, Sheng 2017)
Spasticity results from hyper-excitability of the stretch reflex, which gradually develops after stroke.
It is attributed to disinhibition of stretch reflexes as a result of altered descending inputs to spinal stretch reflex circuits after stroke.
Dorsal RST descends in parallel with CST in the dorsolateral funiculus and provides a dominant inhibitory effect on the spinal stretch reflex, while medial RST and VST descend in the ventromedial cord, providing excitatory inputs. (It is important to note that dorsal RST receives facilitation from the motor cortex via corticoreticular projections, which run in close proximity with the corticospinal tract).
In stroke with cortical and internal capsular lesions, damages often happen to both CST and corticoreticular tracts due to their anatomical proximity, resulting in loss of cortical facilitatory input to the medullary inhibitory centre, thus less inhibition from dorsal RST. This leaves the facilitatory medial RST and VST unopposed, since they are independent of cortical control, thus the stretch reflex hyperexcitability.
This mechanism could also explain why a stereotyped pattern of spasticity is observed regardless of affected areas (cortical or subcortical stroke).
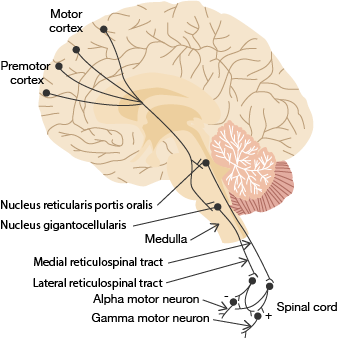
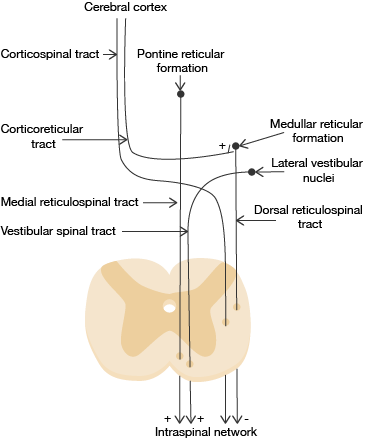
Systems involved in spinal reflex excitability in spasticity
Diagram explanation:
The lateral RSS is excited by the cortex (corticoreticular tract), this causes the lateral RSS to be inhibitory to the spinal reflex.
The medial RSS and vestibular tracts are excitatory, they are not under cortical control.
Therefore when there is cortical/ higher level damage the influence on to the lateral RSS is lost, this means there is less or no inhibition, and the excitatory medial RSS and vestibulospinal tract have no opposition and the spinal reflex becomes hyper reflexic.