Note that the son and wife are not in agreement about the best course of action. This can be very difficult for everyone involved and it sometimes requires several meetings to reach consensus
A key theme here is ‘unrealistic expectations’ (from the son)
Note that the son appears to have changed his mind about how actively his father should be managed
Remember that all this information needs to be shared with the team. The discussion should be carefully documented in the notes and accessible to members of the multi disciplinary team. The son may approach other staff and a consistent message should be given
Derek White a 75-year old man is now 6 weeks post a left total anterior circulation infarct (dense right arm and leg weakness with aphasia) with no recovery of the initial severe deficit. He is NG fed and cannot talk or walk. He is doubly incontinent. The chances of him making a recovery to independence are poor.
He has had 3 aspiration pneumonias and develops a 4th episode. The on call team have started antibiotics.
You feel that further episodes of life prolonging antibiotics may not be in his best interests as the chances of recovery are poor.
His family have already been informed.
His wife had previously indicated that she felt that he’d ‘had enough’ and should be allowed to die peacefully.
His son, who had up until now been content with the care his father had been receiving, and seemed to be aware that his father might not survive, now wants everything possible done and thinks that ‘if he just had a bit longer with feeding and one more course of antibiotics he will start to recover and get back home’.
The patient in this case is fictional but based on real cases. The following video contains still images and audio. If you are having issues with opening the interactive video, please follow one of the alternative video links below.
For further discussion about how to describe the dying process, see next case.
Families should be informed about what is likely to happen when the patient is close to death e.g. ‘rattly chest’ erratic breathing, less need for fluids, skin becomes discoloured etc.
Should continue to be explicit about which treatments will and will not be given and why.
Find out whether the family would want a night call if the patient dies in the night-and document this in the notes.
Explore whether the family want there to be a family member present at all times-some families like to have a ‘rota’ system so that there is always someone there. Note this needs to be balanced against the need for families to have respite and rest.
The medical team should continue to include the patient in the ward round and talk to the family regularly even if these updates are very short.
If family are present at the time of death, explain that it is OK for them to hold the person’s hand or talk to them as they die. It’s OK and sometimes desirable for them to be present when a doctor certifies death.
Chaplaincy services can be contacted if relatives request this or if they are very distressed and want to talk to someone not involved in the medical or nursing care.
General Points about discussions about ‘goals of care’
In the ‘first few hours’ scenario, we explored how to have conversations with families whose loved ones were going to die within a few hours of a stroke. Often though patients deteriorate slowly after stroke and the dying process can be more prolonged. Sometimes it is difficult to be certain whether a patient is dying – recent NICE guidelines provide some useful guidance.
In this case scenario the team is almost certain that the person will die within the next few days:
Note that the term ‘Withdrawing treatment’ can be perceived by family as ‘withdrawing care’. So it’s best to avoid using the term ‘withdrawal of treatment’ but instead use the phrase such as ‘providing care and stopping unnecessary treatments that aren’t working’. This might include stopping artificial feeding (which is considered a ‘treatment’) stopping intravenous fluids, stopping life prolonging treatments especially when they are distressing for the patient, investigations e.g. blood tests, radiological tests, secondary prevention of stroke.
Conversations about the possibility of stopping treatments should ideally have begun at the time when the treatment was started and may have adopted time limited interventions with agreed criteria for stopping treatments.
Involve the patient if possible and all relevant family members with clear dissemination strategies to other members of the family who might not be present and to other members of the team.
Could be a shared decision with patient and family.
It is important to establish whether a family member has a legal role in decision making e.g. Power of Attorney; if the patient cannot communicate.
Should cover future plans for symptom control.
Should be explicit about which treatments will and will not be given. Acknowledge that all decisions will be reviewed to determine if still appropriate.
You should be explicit about whether or not you will continue to do observations. If you stop observations the family may feel that you are no longer monitoring the patient.
Patients’ currently or previously expressed wishes should be taken into account.
Second opinions may be sought and can be useful.
Should include a discussion about preferred place of dying e.g. hospital or home or nursing home-staff may need to bring this up as families are often reticent about asking. Staff should explain clearly if they feel the person is too ill to be moved even if the family would have preferred care at home.
Making decisions about nutrition and hydration is complex and we need to understand the complexity
Receiving nutrition and hydration may be life sustaining but we can then be at risk of prolonging a very poor quality of life
We need to listen carefully to appreciate the perspectives of the people involved. These may be due to personal values, interpretation of information or emotional reactions. Risk versus benefit for any decisions should be clearly documented.
Rushed or ill-informed discussions can have a lasting impact
We need to document what we have discussed, what we are doing and explain decisions to allow the multi-disciplinary team to provide a consistent approach
Decisions will be on a case by case basis taking full account of the person’s and family’s wishes but within both legal and best practice guidelines
Offering oral intake for comfort at the end of life is considered basic care and when a person is unable to take anything orally, ensuring they receive adequate oral care is paramount. Treatment approaches can change quickly and when a person transitions from active treatment with alternative nutrition e.g. Nasogastric Tube under a “Nil By Mouth” recommendation due to unsafe swallow, to a palliative treatment approach, where alternative nutrition is removed, their ability to accept some oral intake for comfort should be reviewed promptly.
Families may require psychosocial support and an understanding of why appetite diminishes and why oral intake may change towards end of life. While swallowing difficulties can have a significant impact, other factors such as change in taste, loss of smell, loss of appetite, change in bowels, nausea can all impact (RCP, 2021)
When a person has capacity, or has previously stated their wishes regarding eating and drinking, or a best interest decision regarding eating and drinking has been made, and a decision is made that may seem unwise to others e.g. eating and drinking with acknowledged risk, as long as their carers who act upon their request have acted with due care, they should not be exposed to any liability if the person, does, in fact, suffer adverse consequences. (RCP, 2021).
If the patient develops any complication of thrombolysis
Stop the Infusion
Seek urgent medical assistance
Increase frequency of monitoring
Here are some links to protocols which have been suggested for managing complications of thrombolysis. However, you may have local protocols for managing complications – you should familiarise yourself with these:
Angela does not suffer any complications, and the following day her weakness is very mild, although she still has a visual field defect. She is discharged home after three days to continue her rehabilitation with the early supported discharge team.
Key message
Thrombolysis increases the chances of a good recovery
All patients and families should have thrombolysis treatment explained clearly to them, including the benefits and risks
Monitor the patient to detect any early signs of complications. These most often occur during, or within hours of finishing, the infusion.
Safety of the patient following thrombolysis treatment is very important; especially if the patient has sensory inattention or neglect. Simple measures such as avoiding wet shaving helps minimise the risk of minor bleeding.
Falls prevention
Moving the patient to a more observable area of the ward should be considered to minimise the risk of falling. A fall could result in intra-cranial or extra-cranial bleeding and/or injury. Hazards should be identified: agitation, restlessness, confusion, nicotine and alcohol withdrawal. Consider using a falls assessment tool e.g. Cannard, Tinnetti, Falls Risk Assessment Score; if your patient has a fall please inform medical staff immediately – note any bleeding, new bruising or injuries.
Medication
Avoid aspirin, clopidogrel, heparin, warfarin or non-steroidals for 24 hours after thrombolysis – these can be considered after 24 hours if there is no evidence of bleeding. Some medication may increase the risk of bleeding following treatment including non-prescription drugs.
Invasive procedures
Procedures such as catheterisation, injections, nasogastric tube, arterial punctures, central lines or lumbar punctures should be avoided for 24 hours after thrombolysis. Care should be taken when removing indwelling intravenous catheters as there may be excessive bleeding.
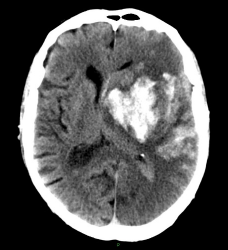
Extensive bleeding (white) into an area of cerebral infarction
This CT scan shows extensive bleeding (white) into an area of cerebral infarction. This is known as haemorrhagic transformation of an infarct (HTI).
Monitor the patient to detect any early signs of complications. These most often occur during, or within hours of finishing, the infusion.
A baseline set of NEWS (National Early Warning Signs) observations including temperature, pulse, respirations, blood pressure, oxygen saturation, blood sugar, Glasgow Coma Scale and NIHSS should be obtained and recorded prior to starting the infusion. During the infusion monitor for changes, initially every 15 minutes for two hours, every 30 minutes for the next 6 hours and hourly for the next 24 hours but this may be varied, depending on the patients condition. Use a manual blood pressure cuff to help reduce bruising and monitor the patency of the intra-venous line during and post infusion.
Observe for signs of:
Intracranial bleeding:
Headache and/or vomiting
Drowsiness
Increase in NIHSS
Irritability / agitation
Seizure
Extracranial bleeding:
Falling blood pressure and rising pulse
Bleeding from any orifice (mouth, rectum, nose, urogenital tract)
Pain, bruising or swelling, especially in joints, muscles or abdomen
Associated with any recent injury, cannulae or operation site