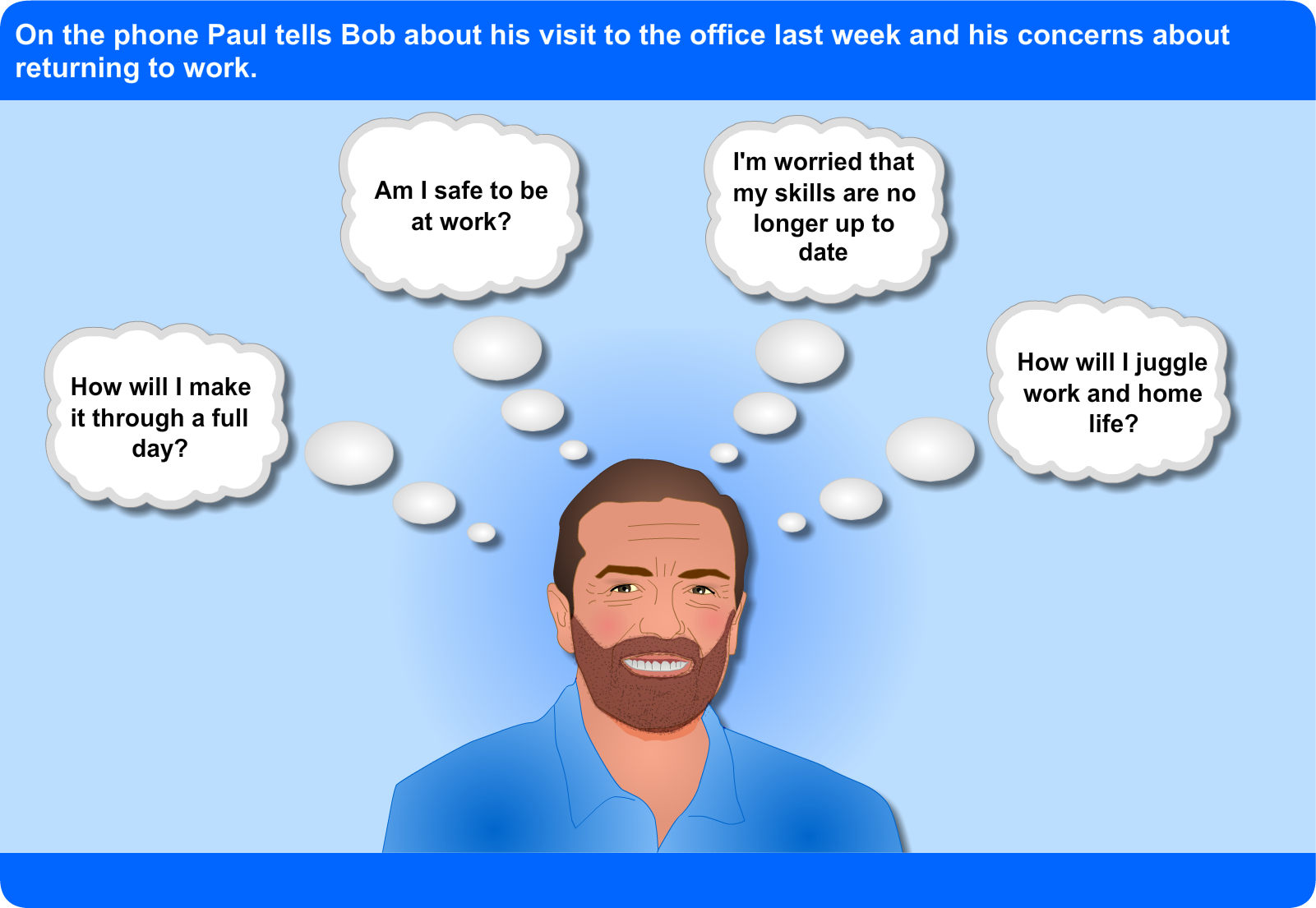
The next day, Bob sets time aside to return Paul’s phone call. First he provides Florence with some background information. He is a 47 year old IT support service engineer, who lives with his partner and two children and is now 10 months post stroke. Paul is coping well and feels as his days are busy he is now ready to return to work. He has an active caring role for his children and has taken on more of the household chores whilst his partner works. Paul occasionally attends his local gym, gets his daily paper from the corner shop, completes the crossword and Sudoku to keep his brain active and is glad to be back driving.
Bob tells Florence that since his stroke Paul has demonstrated good understanding of his condition and has the skills to manage it. Bob explains that Paul knows and practices his home exercise programme, is good at pacing himself, uses goal setting to break down more complex tasks, looks after his health – has managed to stop smoking with the help of his doctor; makes sure he attends for routine medical check ups for his BP and knows when to seek advice. Bob has not had any input for several months but is comfortable with him making contact now.
When Bob arrives, Jenny and Angus are both there. Angus tells Bob ‘I’ve had a fall and couldn’t get up, it was so embarrassing. I don’t feel so good on my feet now but before this was out walking two miles every day, it was tiring but it was doing me good. I have only been to the stroke club once but I’m not sure about it. At least I’ve lost some weight.’
Jenny tells Bob again how difficult she is finding the current situation and is concerned that her Dad is socially isolated. Whilst acknowledging the setback Bob emphasises the positive achievements Angus has made since going home.
Later that day, Bob and Florence go to see Angus. In the car Florence looks through Bob’s notes from his last visit.
 |
Background: Angus McLeod had a mild left hemiparesis. He is a retired police officer who previously enjoyed golf and socialising. He lives alone but is supported by his daughter Jenny who lives nearby. His general health is good though he does have a history of hypertension and is overweight.
1st visit: Goals identified
- Reduce risk factors by losing weight and increasing activity levels
- Increase fitness levels to return to golf
- Increase social activity by attending local stroke group
- Build confidence going out to meet friends at golf club
Outcome: Mood screening completed – no issues identified. Happy with goals and next steps. Plan: visit in one month.
2nd visit: Goals reviewed
- Losing weight and feeling positive about this
- Getting out walking most days and pacing this well
- Not yet made it to the stroke club but planning to go next week
- Set a date to meet friends at the golf club for a drink
- Having been signposted to the CHSS self help 4 stroke website and is now working through the resource
Outcome: Angus is coping well. Plan: visit in one month.
Current: Frantic phone call from daughter, Jenny highlighting new issues that are worrying her.
She reports that her Dad fell at the golf club and has completely lost his confidence so that he is not going out at all now. He only went to the stroke club once and appears very down and withdrawn. He does not appear to have the energy to do things anymore. She says she has tried talking to her Dad about these issues but feels she is getting nowhere. She requests that I come and see her Dad as soon as possible. |
Florence watches as Bob supports Alice and Sid in setting new goals.
Alice, Sid and Bob begin first by discussing and documenting Alice’s new priorities.
- She wants to have a clear role in her own home as she used to, contributing to shopping, laundry and cooking.
- She feels able to go to the toilet herself and wants her husband to allow her to do that
- She wants Sid to meet up with his friends and get his life back
- She wants to meet friends for lunch without Sid coming too
Based on these priorities they then set and agree new goals and what steps are needed to complete them.
| Date |
Goal |
What will I do? |
Review Date |
| 23-10-20 |
I will have more control in the kitchen and make all meals |
- I will organise and write the weekly shopping list
- I will start with simple pre-prepared meals
- For more complex meals I will plan to spread the tasks through the day
- I will fill the dishwasher and put the washing on
- I will ask Sid for help if I need it
|
23-12-20 |
| 23-10-20 |
I will go to the toilet without Sid helping or coming with me |
- I will tell Sid when I am going to the toilet
- I will shout if I need help and leave the door unlocked
- I will make sure that I leave enough time to do this myself
|
14-12-20 |
| 23-10-20 |
Sid will leave me alone in the house for a morning twice a week and go out with his friends |
- Sid will go out for a short periods twice a week and build up his time away
- I will make sure that I have all I need before he leaves
- When he goes for his first full morning away I will invite a friend round
- I promise to phone Sid if I need him
|
22-12-20 |
| 23-10-20 |
I will organise and go out for lunch with my friends without Sid |
- I will start by going for coffee with friends and initially Sid will take me, leave me and pick me up
- I will start to book a wheelchair taxi for my trips out and go without Sid
- I will gradually build up my time out
- I will have lunch in a restaurant that I know has suitable access and toilets
|
22-12-20 |
Alice and Sid tell Bob that they can see how goal setting will really help them cope with their challenges at home and allow them to make tasks more manageable. They also tell him that they feel more confident about what to do but would like him to help them with it again. Bob reassures them that he is happy to do that but he feels sure they will soon be able to do it by themselves.
Bob has been visiting Alice for two months now. See Bob’s diary at the end to find out how Alice and Sid are doing.
| Support |
Refer |
Information |
Explore:
- Strategies to cope with therapy withdrawal
- Changing roles and relationships
- Impact of stroke on their emotional well being
|
Discusses referral options
- Local counselling service
- Wheelchair exercise group
|
Provides written information on
- Stroke e.g. factsheets
- Local carers group
- Stroke support group
- Stroke4Carers website
- Wheelchair accessible transport
|
Together they decide that goal setting would be an excellent starting point for supporting Alice and Sid to self manage effectively. Whilst they have a chat about what goals they would like to set Florence asks Bob what the differences are between hospital and community goal setting.
Bob introduces Florence to Alice and Sid and asks Alice how things are going generally. Alice is pleased to be home but appears to be quite stressed and low in mood.
| Alice |
Sid |
|
 Bob explores with Alice what the problems are. She tells him … Bob explores with Alice what the problems are. She tells him …
‘Goal setting in hospital really helped me focus on what I needed to do to get home. But it seems difficult now my priorities are so different – I can’t do it alone.
‘My husband is frightened to leave me on my own. It’s putting a strain on our relationship, I feel such a burden to him.
‘The community rehabilitation team tell me that they stop after 6 weeks – what happens after that? How will we cope?
‘I’ve lost all the roles I used to have in the house and it’s really frustrating. Our lives seem so focused on my illness now.’ |
 Bob wonders what Sid’s thoughts are on how things are going. Whilst Florence is talking to Alice, Bob takes the opportunity to chat to Sid who tells him … Bob wonders what Sid’s thoughts are on how things are going. Whilst Florence is talking to Alice, Bob takes the opportunity to chat to Sid who tells him …
‘I was really looking forward to Alice being home but I didn’t realise how hard it would be.
‘Everything takes so much longer now, that’s why its quicker if I just do it for her.
‘Nobody told me a stroke would end our social lives. I never get out on my own now and as for holidays that’s never going to happen.
‘I can’t leave her alone in the house, I mean what if she fell or had another stroke? It’s just easier if I stay in and watch her.
‘How will we cope when the community rehabilitation team leave? Surely she needs more therapy, she’s not back to normal yet.
|
| Bob |
 |
Having listened to what both Alice and Sid have told him Bob identifies the main issues to address:
- Alice requires to take control of her life and self manage her condition
- Sid needs to come to terms with his wife’s stroke and given some encouragement to let Alice do things for herself
- Alice is struggling to transfer her goal setting skills into the community
|
Bob and Florence talk through the self management strategies available to him. Bob thinks the key ones for this situation would be education, provision of information, referral to other services and goal setting.
Prior to going to see Alice, Bob explains to Florence that she is a 68 year old lady who had a stroke whilst on holiday abroad. Alice was transferred back to the rehabilitation unit where she spent 4 months and has been home for just over three weeks. He tells Florence that the hospital handover indicated that Alice actively engaged in goal setting as an inpatient and was very keen to continue with it once home.
This is Bob’s second visit, the first was really to introduce himself and get a little background information. His aim today is to work with Alice and her husband Sid to continue building on existing skills and gain additional abilities to self manage.
Bob takes Florence through his diary for Monday and Tuesday of this week.
Bob tells Florence that he hopes she will get an understanding of the following during the week:
- What self management is
- Which approaches are commonly used in the community
- The professional’s role in self-management in the community
- How goal setting applied in the community differs from that used in the hospital setting
- How self management approaches, like other treatment interventions, need to be tailored to the individual
Bob and Florence prepare to go and see Alice Rowan.