Category: Topic Loops
Carotid intervention
Introduction
Atheromatous narrowing, or stenosis, of the internal carotid artery is a common cause of stroke and TIA. It can be identified radiologically using a number of vascular imaging techniques, including Carotid Doppler Ultrasound, and CT or MR angiography.
Carotid endarterectomy is an operation to remove an atheromatous narrowing of the internal carotid artery. This removes the source of embolism and reduces the risk of future stroke. Surgery is generally considered for patients with TIA or non-disabling stroke due to stenosis of more than 50% in the symptomatic vessel. If the carotid artery is completely occluded surgery is not required.
Carotid angioplasty and stenting: a balloon inserted via an artery can be used to stretch the narrowed artery. A stent can then be inserted to keep the artery open. Carotid angioplasty and stenting is an alternative option to surgery. It is less invasive than open surgery but is not always as effective. It can be considered for patients who are not suitable for open surgery.
The risks and benefits of any intervention (surgery or stenting) need to be carefully considered and discussed with the individual patient. These procedures are used in addition to standard medical treatments. Reference: Royal college of Physicians Stroke Guidelines (2016).
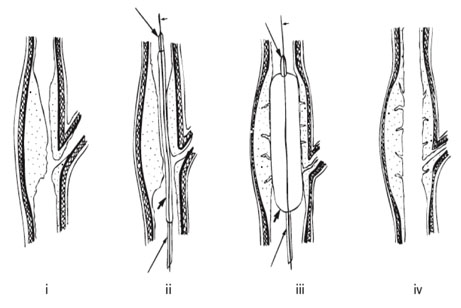
Diagram to show the principal of angioplasty: (i) the carotid bifurcation with severe atherothrombotic stenosis; (ii) the guidewire (small short arrow) with the deflated (short thick arrow) balloon catheter (long arrows) is passed across the stenosis; (iii) the balloon is inflated and the plaque is pushed outwards, so stretching the arterial wall and cracking the plaque; (iv) after the balloon is deflated and removed, the lumen has been widened, the arterial wall remains stretched and the plaque remains.
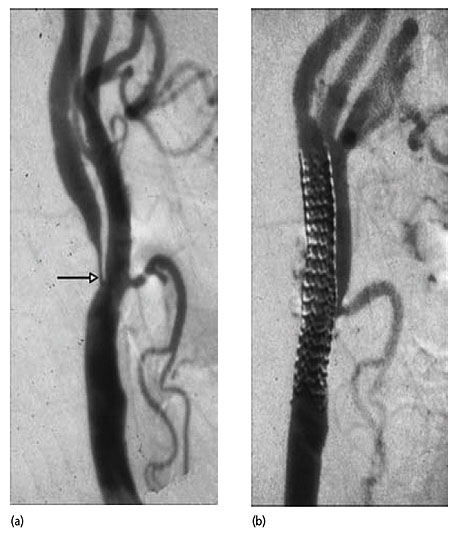
Catheter angiogram before (a) and after (b) stenting; before stenting there is a severe stenosis of the internal carotid artery (arrow) and afterwards the mesh of the stainless steel stent can be seen spanning the carotid bifurcation (modern stents are not so easily seen). (Courtesy of Prof Martin Brown, London)
Links and references
- NICE
- Prochaska J, O., DiClemente C.C. The transtheoretical approach: crossing traditional boundaries of therapy. Home wood, Illinois: Dow Jones-Irwin; Dow Jones-Irwin Dorsey Professional Books.1984
- Readiness to Change Ruler
- http://www.healthscotland.com/
What is my role when providing a brief intervention?
How do I carry out a brief intervention?
Application to the secondary prevention of stroke: lifestyle issues
- The effectiveness of brief interventions has been demonstrated in relation to lifestyle risk factors for recurrent stroke, namely:
- Tobacco use
- Alcohol and other harmful substances
- Unhealthy diet
- Physical inactivity
- Brief interventions may be used effectively by a range of healthcare professionals, working in a range of healthcare settings
Key characteristics
- Typically, a brief intervention takes between 5 and 10 minutes
- A brief intervention may include one or more of the following:
- Health education and advice
- Assessment of what stage an individual is at (Stages of Change model)
- Practical support
- Behavioural support
- Provision of self-help information
- Referral to advice/support lines
- Referral to specialist services e.g. smoking cessation services
Brief interventions
Introduction
- Brief interventions may be used to give individuals an opportunity to consider their lifestyle behaviours and the effect these behaviours may have on their health
- Brief interventions may:
- Be used by a range of healthcare professionals
- Involve the provision of opportunistic advice, discussion, negotiation or encouragement
- Range from offering simple, generalised advice to more extensive individualised advice
- May consist of one session or several
- Brief interventions are easy to implement, and are a cost-effective health promotion tool
Blood pressure reduction Quiz
Benefits of blood pressure reduction
Press Play to watch the animation.