This is the module test for ‘HEARTe 4. Acute coronary syndromes’. It is strongly recommended that you work through the learning materials of the module prior to commencing this test. By going straight to the test you may miss out on valuable learning contained within the module. The answers to all the test questions are contained within the module. This information may have been provided in the ‘Additional Information’ boxes on some of the pages.
There are 10 questions and you must answer all of these correctly to obtain a certificate of completion.
You should allow approximately 10 minutes to complete the test.
On completion of this case you should have an understanding of:
The Electrocardiogram (ECG) changes in ST Elevation Myocardial Infarction (STEMI) patients: Most patients will have ST segment elevation, but new left bundle branch block can also be seen. Since there are other potential causes of left bundle branch block, is important to consider the patient history and if possible to review old ECG”s.
The initial monitoring and treatment that may be undertaken by paramedics prior to transfer to an intervention centre.
The fact that a cardiac arrest is not uncommon in myocardial infarction and requires immediate life support from either bystanders or health care professionals.
That primary Percutaneous Coronary Intervention (PCI) is the treatment of choice provided the patient can be transferred to the appropriate centre within 120 minutes of attendance by the ambulance service.
After transfer to CCU, Naveed asks the nurse why he has sore ribs. The staff nurse explains that his heart stopped in the ambulance and he needed CPR and an electric shock to start it again. Naveed then looks really anxious and asks whether this will happen again and starts to cry. The nurse provides him with information about what causes heart attacks, what treatments are necessary and how Naveed can begin the process of getting back to normal.
She explains that it is a normal reaction after a cardiac event or procedure is to feel anxious and emotional and during further involvement with cardiac rehabilitation this will be explored and monitored as appropriate.
Naveed is monitored for the next 12 hrs and prescribed regular post MI drugs. He has an echocardiogram the following day which shows no significant damage to his heart. He is moved to another cardiac ward where he has more contact with other patients and begins to mobilise.
During this time he meets the cardiac rehabilitation team and learns more about his recovery and is ready for discharge a few days after this. Both he and his family have lots of questions about his heart attack and the cardiac rehabilitation nurse also gives him booklets to help them retain and understand all of the information he is given. The ward pharmacist reviews his medication and gives him more information regarding this.
A repeat 12-lead ECG taken after coronary intervention showed resolution of the left bundle branch block indicating a successful procedure. Naveed was then transferred to a coronary care unit bed for ongoing monitoring.
His radial artery compression band was removed after 4hrs with haemostasis achieved and the tirofiban infusion was continued for a further 12 hours.
In the cath lab, the nurses start Naveed on an infusion of tirofiban (a powerful anti-platelet drug). A sheath is inserted into his radial artery and an angiogram is performed that shows an occluded left anterior descending artery. An angioplasty guidewire is passed through the catheter to the blocked artery and advanced across the blockage. A thrombus aspiration catheter is fed over this wire, and thrombus removed from the artery by suction. This restores flow to the artery and a bare metal stent is implanted in the artery to complete the procedure.
En route to the royal infirmary Naveed loses consciousness and the cardiac monitor shows Ventricular Fibrillation (VF). The cardiac monitor also shows that Naveed’s other cardiac observations have deteriorated and the alarm has been activated.
Paramedics note that Naveed has developed VF and begin Cardiopulmonary Resuscitation (CPR). Following a single 150 Joules (J) shock, sinus rhythm is restored and Naveed regains consciousness. Here are links to resuscitation council guidelines for Basic Life Support (BLS) and Advanced Life Support algorithm (ALS).
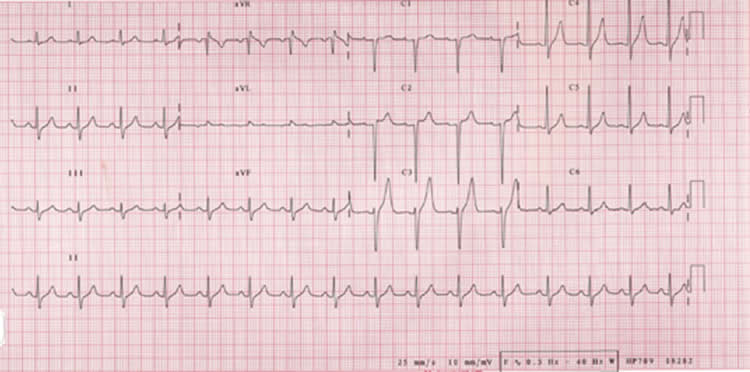
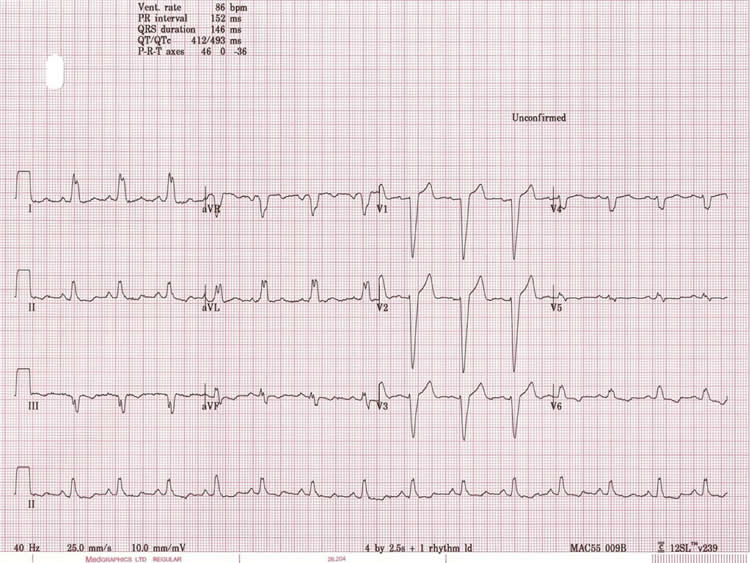
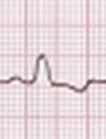
The paramedics arrive and perform a 12-lead Electrocardiogram (ECG). This shows left bundle branch block (LBBB). The ECG is telemetred to the Royal Heart Infirmary who advise transfer to the cath lab for immediate primary angioplasty. The paramedics are told that Naveed has received aspirin 300mg, so give him clopidogrel 600mg (both orally) and heparin 5000 units (iv) after establishing intravenous access. Oxygen is administered as Naveed’s saturations are low.
Left bundle branch block is caused where there is delayed depolarisation of the left ventricle. On the ECG this is seen as a lengthening of the QRS complexes. It can be a sign of an acute ST elevation MI.