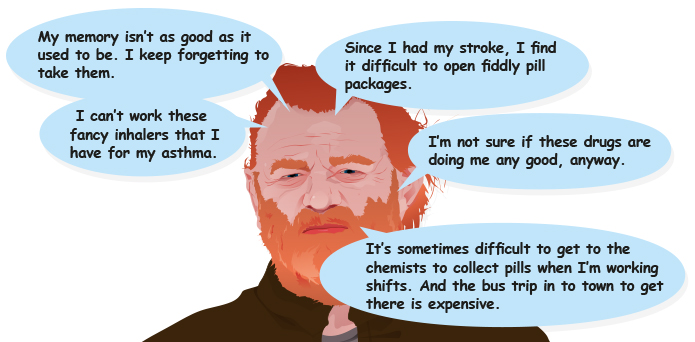
Sandy’s GP arranges for him to meet with the Heart Failure Nurse at the health centre. One of the main issues that individuals with multiple conditions often encounter is polypharmacy. Sandy is on a range of medications for his different conditions. The Heart Failure Nurse has three main questions she wants to ask Sandy:
what medication is he currently on?
is he taking his medication?
how can he be supported to adhere to his drug regime?
Please enable JavaScript in your browser to see this interactive content.
Is Sandy taking his medication?
Sandy admits to the heart failure nurse that he hasn’t been taking his medications as prescribed.
How can Sandy be supported to adhere to his drug regime?
The heart failure nurse explains to Sandy what each drug is for and reinforces the importance of taking them regularly. She notes down a number of actions that may improve Sandy’s concordance. (For further information on concordance, please see Additional Information, below.
Sandy and the Heart Failure Nurse also discuss potential health behaviour changes that he might like to consider.
Please enable JavaScript in your browser to see this interactive content.
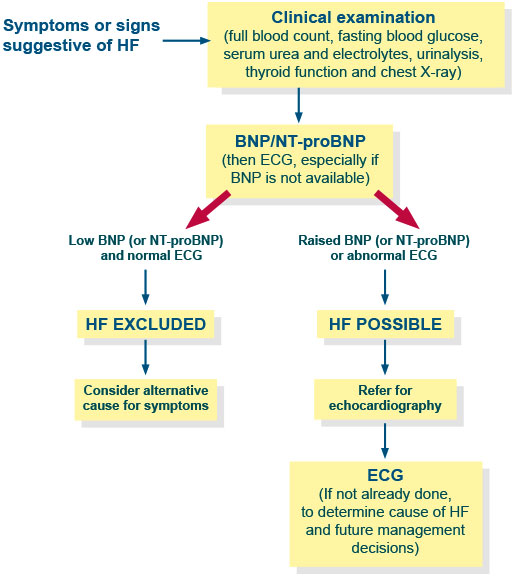
Sandy manages to organise financial support through the Cash in Your Pocket scheme and travels to Aberdeen to meet with the cardiologist. The cardiologist assesses Sandy using an algorithm for diagnosing chronic heart failure. SIGN 147 Management of chronic heart failure, 2016
Sandy undergoes the following investigations, in addition to the blood tests carried out by his GP:
Please enable JavaScript in your browser to see this interactive content.
Sandy is diagnosed with heart failure, NYHA II. After discussion with Sandy about his test results, the cardiologist refers him to the Heart Failure Nurse.
Please enable JavaScript in your browser to see this interactive content.
The GP asks the Practice Nurse to take blood samples from Sandy to test for:
full blood count
urea & electrolytes
liver function tests
thyroid function
glucose
HbAlc
The Practice Nurse also asks Sandy to do a Peak Flow test. This is a test that provides an objective measure of how his lungs are functioning. It is done as a routine check on individuals diagnosed with asthma. Sandy’s peak flow readings are significantly reduced compared to the last readings taken. The GP suspects that Sandy is suffering from heart failure, however, he needs to ensure that Sandy’s breathlessness is not caused by poor control or deterioration in his asthma.
The GP explains to Sandy that he would like to discuss his case with medical staff at the nearest acute hospital and tells Sandy that he will contact him once he has done this. He tells Sandy about the Cash in Your Pocket scheme that is available in to individuals living in the area and to which Sandy can apply to for financial support to pay for his visits to the various clinics he needs to attend. Sandy agrees this seems a good idea and the GP fills out a referral form for him.
Sandy suffers from a number of conditions, all of which impact on the health of his heart.
Atrial Fibrillation
Atrial fibrillation (AF) is a heart condition that causes the heart to beat irregularly and too rapidly. If uncontrolled it can lead to long-term cardiac damage, eventually causing ventricular systolic dysfunction, decreased cardiac output, increased ventricular filling pressures and increased vascular resistance. AF is associated with heart failure and the two often occur together. The combination of the two is related to increased morbidity and mortality compared to each disorder on its own. Although the relationship between AF and heart failure is not fully understood, it can be explained, to a certain extent by the presence of the same risk factors, of which diabetes is one. The prevalence of AF is spreading, along with the growth of the elderly in the general population. Sandy’s diabetes may have been a contributory factor in his AF.
Sandy has type 2 Diabetes Mellitus. Diabetes is regarded as the strongest risk factor for heart failure. The prevalence of diabetes in heart failure patients is close to 20%, compared to 4-6% in the general population. This increased risk is associated with a number of different factors. Diabetes is known to accelerate the development of coronary atherosclerosis. People with diabetes have an increased level of low-grade inflammation of arterial linings. These initiate blood vessel changes which can, ultimately, lead to heart failure. Diabetics, particularly those with type 2 diabetes, have higher level of th blood fats, including cholesterol, which can lead to cardiac problems. It is also thought that there may be a specific cardiomyopathy that contributes to heart failure and makes diabetic individuals more liable to develop the condition.
Asthma
Asthma is a respiratory condition marked by attacks of spasms in the bronchi of the lungs, causing difficulty with breathing. It is often associated with allergens and allergies to particular substances. Although asthma is associated with an increased risk of heart failure, the reasons for this are unclear. There may be a link between the inflammatory processes that occur in asthma and those that take place in heart failure but this link is not fully understood. There is some evidence, also, that the medications taken to prevent and treat asthma may be implicated in the development of heart failure, particularly if an individual is taking multiple medications.
Taken together, Sandy’s AF, type 2 diabetes and asthma put him at increased risk of developing heart failure.
Sandy is a 48 year old man, who has been diagnosed with atrial fibrillation, type 2 diabetes and asthma. Due to his multiple conditions, Sandy has had to discontinue his previous work as a trawlerman. Despite having drug and alcohol dependency problems, Sandy has held a part-time job in a local public house for the past few years.
Sandy has no relatives living nearby and his friends are mainly those who regularly visit the pub where he works.
For the past couple of weeks, Sandy has been feeling generally unwell so he decides to visit his GP.
This module will focus on two individuals, Sandy and Mina, both of whom have heart failure along with other, multiple conditions.
Sandy is newly diagnosed with heart failure and is at the beginning of the heart failure illness trajectory (NYHA II), whilst Mina has had heart failure for some time and is further along this trajectory (NYHA IV). Their multiple conditions have a major impact, not only on the course of their heart failure, but also on the management of their conditions.
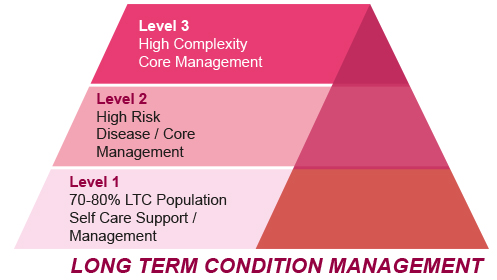
Supporting self management is recognised as being a core part of high quality care for people living with LTCs. Far from leaving the individual with a sense of being abandoned, supported self management empowers people to harness their knowledge, skills and resilience, and seek access to care and support which addresses their own specific needs (Taylor et al, 2014). Although health care professionals play an important role in the enhancement of self management skills, it is the individual’s access to social support which often ensures changes are implemented and sustained. Self management requires the establishment of a partnership which empowers the individual through the development of key skills and understanding. Self management is multifaceted involving physical, psychological and social care. It is estimated that approximately 70-80% of patients with LTCs are able to self care with support (Department of Health, 2005) (Figure 2). The most frequently implemented aspects of self management support are related to education and psychological care (Taylor et al, 2014).
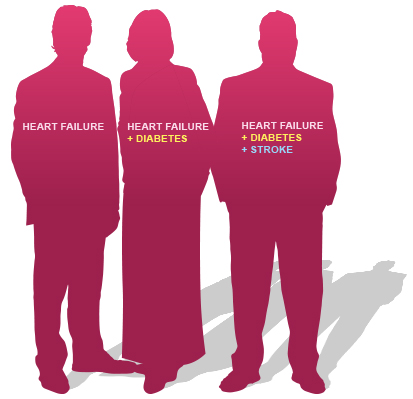
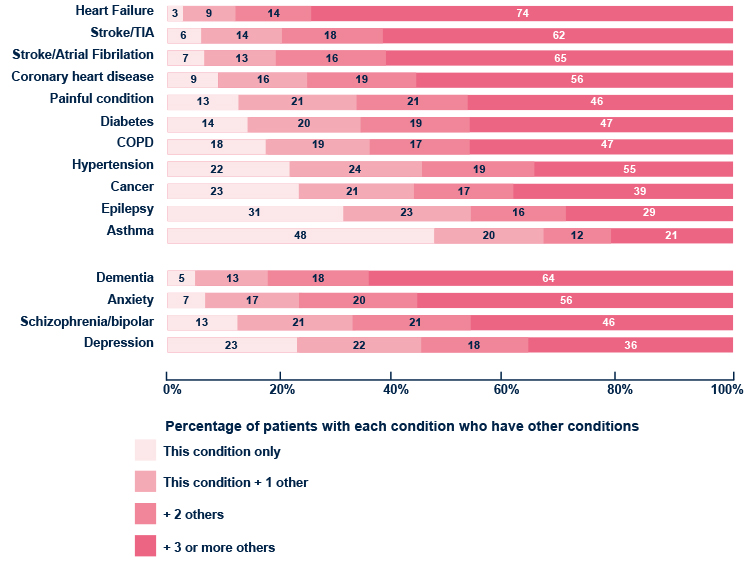
The care of patients with multiple medical conditions is one of the greatest challenges now faced by healthcare providers. To date the vast majority of medical research, guidelines and contractual agreements have dealt with single targets for single disease states, whereas in reality many patients have multiple chronic conditions, requiring multiple treatments. The resulting polypharmacy (use of multiple medicines) can be both appropriate and inappropriate and the key healthcare aim for individual patients is to ensure the on-going safe and effective use of their multiple medicines. Research into the management of patients with multiple medical conditions is in relative infancy.
The graph below illustrates the scale of the healthcare issues presented by multiple conditions.
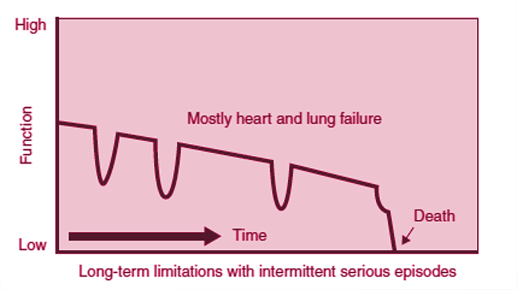
Learning to live with a long-term complex condition can be challenging. Those diagnosed with a progressive life limiting cardiac condition, such as heart failure‚ face living with symptoms which fluctuate, often with episodes of severe deterioration which may lead to sudden death (figure 3). The condition trajectory, therefore, tends to differ from other long term conditions such as cancer, where there is generally a period of decline, or dementia where there is progressive functional deterioration. In this respect, learning to live with ‘uncertainty’ becomes part of the adjustment process.
This Hearte module looks at multiple conditions (where someone is living with more than one-long term condition). In 2014 46% of adults had one or more long-term conditions. The prevalence of long-term conditions increased with age, from a quarter (25%) of adults aged 16 – 24 to three-quarters (77%) of those aged 75 and over (Scottish Health Survey 2014).
Please enable JavaScript in your browser to see this interactive content.
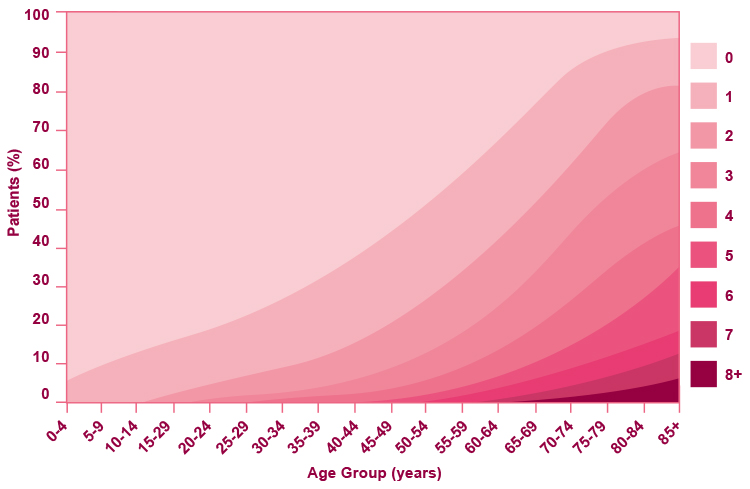
The majority of people in Scotland living with a long-term condition have more than one. By the age of 65 more than 50% of Scots have two or more conditions and the majority of over-75s have three or more conditions. The likelihood of having both a long-term condition, as well as a greater number of them, increases as you get older. Given that the Scottish population is ageing, with the greatest increase being in the oldest age groups, this has major implications for the way we provide health care. According to Harding et al (2013) it is estimated that by 2032 the percentage of the population aged 65 and over will increase by 49%, while those aged over 90 will increase by 148%. Multi-morbidity is more common and occurs at a younger age as deprivation increases. People living in the most deprived areas tend to develop multi-morbidities 10 – 15 years before those living in more affluent areas. In addition, mental health issues are strongly associated with the number of physical conditions that people have.