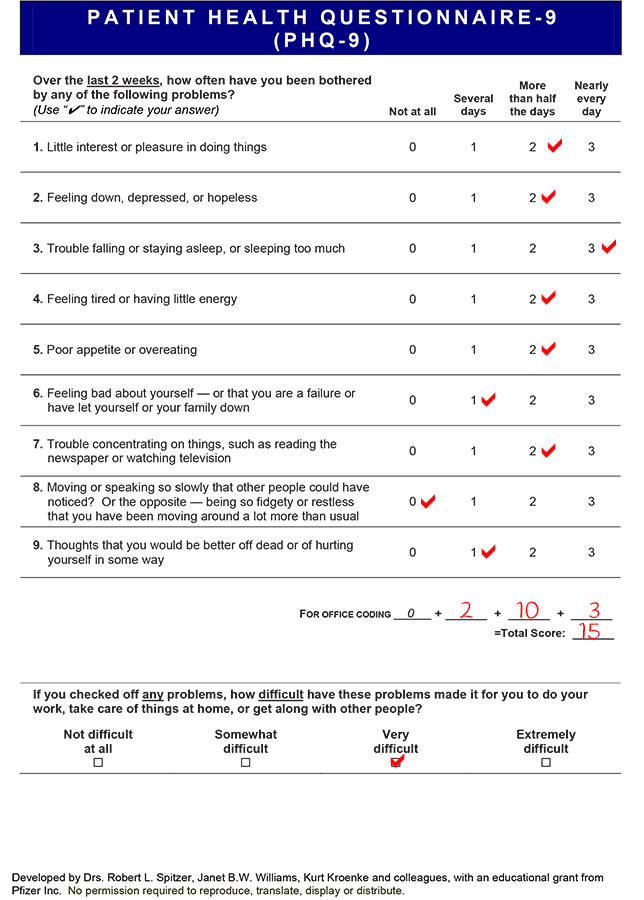
Based on her score, the GP diagnoses Sheila with moderately severe depression. This indicates the need for referral to specialised support services (Step 3 of the Stepped Care model referred to earlier in the module).
It is important to remember that, while screening tools can be useful in indicating the presence of depression, they are not a substitute for diagnosis.
Sheila is worried about her increasing breathlessness and manages to find a neighbour to keep her husband company while she visits her GP.
Her GP practice uses the SWIFT Check Up tool with patients. This tool allows healthcare professionals to “build up a picture of a person’s key relationships, how they are coping, how things are going at work and at home” (NHS Education for Scotland: Emotion Matters ).
SWIFT
Stress/Coping (Stress/Coping/Special support)
How have things been since we last spoke?
Anything significant happened?
How have you been coping?
What have you been struggling with and what have you been managing?
Is there anything specific you feel you need help with at the current time?
With everything that’s been happening how are your spirits?
Stress
Stress, causes, anything else going on that is adding to stress.
Coping
coping?
coping strategies?
Specific support needed?
Important to bear in mind if a person has a history of mental health difficulties or things we should know about that may mean they need extra support for.
**Check mood if any concerns
Work/Home
How are things for you at work?
How have you been managing?
How are things at home?
Illness/LT Condition
How are you getting on with your condition? (current treatment/any difficulties?)
How are you getting on looking after yourself?
Anything the Doctors have said that you are not clear about?
Are you getting enough professional support?
Any difficulties with this?
Any needs we can help with?
Friends and family
How are things with family and friends?
Do you have enough support?
Is there anything big going on or coming up?
How do you feel everyone else in the family is coping?
Are you able to join in and feel involved in family activities as much as you would like to?
Are you able to see your friends?
Things I like to do
What things do you like to do?
Are you managing to do these?
Hobbies?
Interests?
Are you able to do the things that are important to you?
Please enable JavaScript in your browser to see this interactive content.
Sheila is a 76 year old woman who has has heart failure due to left ventricular systolic dysfunction (see Heart Failure module for more information). Sheila was admitted to hospital 2 months ago with increased breathlessness and reduced exercise tolerance but was discharged home, following a medication review. She is normally independent in her Activities of Daily Living (see Pulse Point below) but is beginning to find things a bit difficult. Because of her breathlessness, she cannot shop as easily as she previously could and she struggles to climb the 3 flights of stairs to her flat. She lives with her husband, who has some health concerns, and she normally helps look after him by preparing his meals and helping him with bathing. The couple have a daughter but, as she works and has her own family, she only visits at weekends. Sheila’s daughter has started ordering food shopping online for her parents. Sheila belongs to a local choir but no longer feels able to attend her weekly choir practice, as she is too tired. She misses meeting her friends for coffee and a chat following their choir sessions.
Sheila has missed a couple of appointments with her GP. At her last review she looked a little unkempt and mentioned that she sometimes forgets her medications.
Angus has regularly attended his Cardiac Rehabilitation classes. He has been practising the techniques he was taught on managing anxiety and using relaxation therapy. He has also been pacing himself and gradually returning to work. He continues to have good support from his family and girlfriend and is more open to talking about how he is coping.
Pulse point
Becoming more physically active promotes psychological wellbeing and has a positive impact on quality of life after an MI. The psychological benefits include:
Improved mood
Reduced stress as well as an improved ability to cope with stress
Improved self esteem
Improved body image
Improved sleep pattern and increased energy levels
Improved confidence in physical capabilities
Reduced levels of anxiety and depression
As people experience these positive benefits, their motivation to continue to be physically active improves. Although short term benefits are apparent after as little as a short walk, longer term increases in physical activity patterns are necessary to optimise the therapeutic benefits.
Angus meets with the cardiac rehabilitation nurse, to discuss how they might work together to manage his anxiety. The cardiac rehabilitation nurse assesses Angus as being on Step 2 of the Stepped Care model. The nurse uses a motivational interviewing approach, which involves talking to Angus and helping him recognise the things that will motivate him to manage the anxiety his cardiac event has provoked. See HEARTe Key themes: Applying HEARTe in practice: Communication styles for more on motivational interviewing. It focuses on the gains to be had from behaving in a positive way and on identifying what might encourage (or hold back) Angus” progress.
Angus attends the Cardiac Rehabilitation programme at his local hospital, where he learns how to manage his lifestyle in terms of diet, activity etc. (For more on cardiac rehabilitation please see the Cardiac Rehabilitation module.)
Angus is shown some general relaxation techniques:
One of the strategies Angus learns about is Mindfulness. Mindfulness is a simple, easily learnt approach to relaxing and taking time out from stress or worries. It is an adaptable and very safe skill that can be used as part of normal life. It is safe and effective in managing stress and worry. It has been shown to help with sleeping difficulties and generally helping people feel less driven. Therefore, it has direct applicability to cardiac disease management.
Please watch the video below on mindfulness. Although the video was made for people who had suffered from a stroke, the content offers a good introduction to mindfulness and is equally applicable to individuals with a cardiac condition.
Chest Heart & Stroke Scotland: Being Mindful
Angus is keen to self-manage his anxiety. The cardiac rehabilitation nurse suggests that he may find the following websites useful:
Angus is admitted for a 3rd time to Accident & Emergency, due to chest pain and breathlessness, but is discharged home as medical staff feel his symptoms are anxiety related. However, A&E staff referred him to the cardiac rehabilitation team for early review. Angus is reviewed by a member if the cardiac rehabilitation team. He is assessed using the HADS screening tool which confirms that Angus has high levels of anxiety.
Whilst Angus is out walking his dog his thoughts include:
“Am I having another heart attack?”
“I feel dizzy and lightheaded”
“My heart is beating faster”
“I am breathing faster and shallower”
“I have a funny tingling feeling all over my body.”
“I feel nauseous”
“I feel like I am going to die!”
It is possible that Angus is suffering from panic-like anxiety. The symptoms of panic can very convincingly mimic symptoms of myocardial infarctions. However, there are minor differences.
Symptom
Pain
Panic Attack
Sharp/stabbing
Around heart
Short duration
Myocardial Infarction
Crushing
Centrally located, moves to left arm, back, shoulders, neck
Longer duration
Panic-like anxiety (panic attacks with or without panic disorder) is the most prevalent condition associated with unexplained chest pain in the emergency department. This is a highly treatable condition which may be responsible for a significant portion of the negative consequences of unexplained chest pain, such as functional limitations and chronicity. However, more than 92% of panic-like anxiety cases remain undiagnosed at the time of discharge from the emergency department. (Foldes-Busque, G., Denis, I., Poitras, J., Fleet, R., Archambault, P., Dionne, C., 2013.)
Please enable JavaScript in your browser to see this interactive content.
One night, Angus begins to feel unwell with chest tightness after walking his dog. He tries his GTN spray but it doesn”t help. Angus phones 999 and is admitted to the Accident & Emergency Department.
All his tests for acute coronary syndrome are negative and he is discharged home the next day. Angus is reassured by medical and nursing staff that everything is normal and there is no indication he has experienced a further cardiac event. Despite this reassurance, Angus feels very anxious.
Angus visits his GP after this admission for a general review and to discuss his medications. He informs the GP he is having difficulty sleeping and is lying awake overnight, worrying that he might have another heart attack. He has tried taking warm drinks and reading until he feels sleepy, but is having difficulty relaxing. The GP gives him some general advice about sleeping but does not want to prescribe sleeping tablets at this stage but tells Angus to make another appointment if his sleep pattern does not improve.
There are three main areas that Angus is particularly anxious about:
he is scared of having another heart attack and of dying at an early age, like his father
he is anxious that the stress of his job will cause another heart attack
he is worried that his relationship with his girlfriend will suffer, as he has read that some men have erection problems following heart attack
Immediately after his discharge from hospital, Angus lived with his sister, with good support from his brother and friends. His sister cooked his meals and he undertook only gentle exercise for the first week. Although Angus was slightly fearful, he felt secure living with his sister. At the end of a week, Angus feels well enough to move back to his own house. His sister visits regularly to help with housework and cooking.
Two weeks after his discharge Angus has recommenced gentle walking with his dog and feels he is making some progress in getting back to his normal level of activity.
Please enable JavaScript in your browser to see this interactive content.
After his visit to the Practice Nurse, Angus feels more worried and concerned than he had before his appointment.
People react in different ways to a diagnosis of a heart condition or to living with cardiac disease. It is common to experience a range of emotions such as anger, worry, fear, sadness and irritability. These feelings can be there all the time or come and go. They can be short lived or persist for several weeks or months.
Reaction to a diagnosis of heart disease
Psychological reactions to heart disease
Numbness:
feeling ‘detached
the event may seem unreal, like a dream, something that has not really happened
only in time may this numbness give away to feeling things more intensely
Fear:
of having a heart attack
of re-experiencing intense physical pain
of “breaking down” or “losing control”
of being left alone or having to leave loved ones
Helplessness:
feeling of being powerless
Sadness and grief:
for loss of being healthy
for the feeling of being invulnerable
for any life changes (e.g. giving up a job or hobby)
Guilt:
for being better off than others, for having survived
for having people worry
regrets for things not done
Shame/embarrassed:
for having been exposed as helpless, “emotional” or needing others’ help
Anger:
at what has happened
at the unfairness and senselessness of it all
at any shame or indignities suffered
at other people not understanding
Shock:
feelings of disbelief
questioning “why me?”
Need for privacy:
wanting time alone
Relationship change:
shift in being carer/breadwinner to “being wrapped in cotton wool”
Angus is a 55 year old man who lives alone and who has no dependents. He has a sister, who he is in regular contact with, and a brother. Angus has been in a relationship with a woman for a few months. His father died of a myocardial infarction and his mother from cancer. He works full time as a financial advisor and, although this is a sedentary job, it is quite stressful. He normally enjoys cycling and walks his dog several times a day. Angus has no financial worries and enjoys going on holiday.
Angus experienced intermittent chest discomfort for approximately one month. He initially thought this was indigestion. However, when he developed severe central chest pain, he called an ambulance as he felt unwell with the pain. He was alone in the house at the time. The paramedic suspected a myocardial infarction. On arrival at the hospital, Angus was taken immediately to the cardiac catheterisation unit. It was found he had two occluded coronary arteries. This resulted in Angus having percutaneous coronary intervention and stenting of both the affected arteries. Following the procedure, the cardiologist explained to Angus what had happened to his his heart and the treatment that had been carried out. Angus was given a booklet about myocardial infarction prior to his discharge 48 hours later. He was advised that the cardiac rehabilitation team would be in touch, with an appointment to attend their rehabilitation programme and this would take around 6 weeks to arrive.
Angus is a 55 year old man who had an myocardial infarction two weeks ago. Angus has been readmitted to hospital a couple of time with chest pain but all his tests are negative. He has been fearful to return to normal life.
Sheila is a 76 year old woman who has been given a diagnosis of Heart Failure. She is finding everything a struggle and is having difficult adjusting the changes in her health. As a consequence, she is not socialising as much as previously and is feeling isolated.