“The stigma of mental illness made it difficult for many with long term conditions to reveal the true extent of their emotional distress and have the confidence to seek appropriate help.”
as shown in: The Living Better Project: Key Research Findings
A significant factor in the explanation for poorer clinical outcomes is that co-morbid psychological problems can reduce a person’s ability to actively manage their own physical cardiac condition. For example, problems such as depression are associated with unhealthy behaviours known to be risk factors for the development and exacerbation of cardiac disease, such as smoking and alcohol use. Self-management is at the core of effective treatment for long-term conditions. The Scottish Government has put self-management at the centre of the policy for the approach to long term conditions (Self-Management Strategy for Long-term Conditions in Scotland 2008).
There are a number of useful resources available to help patients self-manage their mental health:
Whichever screening tool you use the score generated should lead to one of four outcomes:
No action
Low intensity intervention (Step 1 of the Stepped Care Model below.)
Medium intensity intervention (Step 2 of the Stepped Care Model below.)
High intensity intervention (Step 3 of the Stepped Care Model below.)
Stepped Care Intervention Model
Step one of the model is the least intensive intervention and is typically provided first. People can step up or down the model according to their changing needs and in response to treatment. the important thing is that healthcare professionals involved in working with individuals with cardiac disease are able to assess and recognise any signs of anxiety or low mood/depression.
Please enable JavaScript in your browser to see this interactive content.
The person may require continued monitoring through repeated screening to ensure access to the right level of care.
Screening is a brief, repeatable means of assessing the presence of psychological distress. Use of a screening tool with all patients can be helpful in identifying low mood/depression and anxiety. It is also helpful in putting mood and wellbeing on the agenda, indicating that “this is something that we are interested in and happy to talk to you about. This is normal. It is part of our job”. The screening tool opens up the potential for a conversation where people feel that they can discuss this again, at any time. “You mentioned last time that you were feeling a bit low. How are you feeling this week/now? Would you like to complete the screening tool again?”
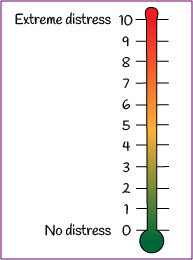
Distress thermometer
A number of assessment and screening tools have been validated and are generally available. The benefit of using an objective screening tool, such as the Distress Thermometer or the Hospital Anxiety and Depression Score (HADS), is because the use of such a tool offers a brief and pragmatic method of identifying patients with psychosocial distress, with the goal of determining who needs referral for more extensive assessment. It is a triage process, to be used in conjunction with your own impressions after speaking to the patient.
Use of a screening tool or standardised questions with all patients at every patient contact greatly increases the chances of identifying low mood/depression and/or anxiety.
People with any chronic physical health condition are significantly more likely to experience mental health problems. The relationship between physical health and mental health is particularly strong within cardiovascular diseases. For example, depression is two to three times more common in a range of cardiovascular diseases including cardiac disease, coronary artery disease, angina, congestive heart failure, or following a heart attack. Anxiety problems are also common in cardiovascular disease.
There are numerous reasons why it is important to effectively manage mental health problems within cardiac care.
Please enable JavaScript in your browser to see this interactive content.
Co-morbid anxiety and depression in individuals with cardiac disease lead to:
Mental wellbeing (also known as emotional health or mental health), can take many forms but a useful description is “feeling good and functioning well”. It describes how we feel and think, and our ability to cope with what is going on in our lives, with its various ups and downs.
“Feelings of contentment, enjoyment, confidence and engagement with the world are all a part of mental wellbeing. Self-esteem and self-confidence are too. So is a feeling that you can do the things you want to do. And so are good relationships, which bring joy to you and those around you” (Professor Sarah Stewart-Brown, University of Warwick)
Jennifer Ritchie, Lead Advice Line Nurse, Chest Heart & Stroke Scotland
Dave Bertin, Voices Scotland Trainer, Chest Heart & Stroke Scotland
Dr Sally Cox, Clinical Psychologist, NHS Grampian
Dr John Sharp, Consultant Clinical Psychologist, Golden Jubilee Foundation
Mairi Smail, Physiotherapist, NHS Dumfries & Galloway
Demonstrate increased knowledge in order to identify commonly presenting mental health conditions related to cardiac disease
Demonstrate an awareness of the bidirectional relationship between cardiac ill health and mental health
Understand a generic model of psychological adjustment to cardiac conditions
Explore self management strategies for facilitating emotional and behavioural adjustment to acute and chronic cardiac ill health
Recognise the signs of severe mental distress and associated risks
Outline appropriate referral systems and pathways for individuals experiencing mental health problems
Discuss the possible pharmacological and non-pharmacological management of mental health problems
General Medical Disclaimer: The information, including but not limited to, text, graphics, images, recommendations, opinions and other material contained on or accessed through this website (or in any module or content accessible through this website) (together “Website”), is intended for general informational purposes only. The information should not be considered as professional medical advice, diagnosis, recommendations or treatment. The information on this Website is provided without any assurance, representations or warranties, express or implied. We do not warrant that the information on this Website is applicable to all healthcare practices, geographical locations, health needs or circumstances. We do not warrant that the information on this module is complete, true, accurate, up-to-date, or non-misleading. You should always seek the guidance of a qualified healthcare professional before making any decisions related to your health or wellbeing. Never disregard or delay seeking medical advice due to something you have read on this Website. The use of or any reliance placed on any information provided on or accessed through this Website is solely at your own risk. If you have any specific questions or concerns about your health, please consult a qualified healthcare provider or other qualified medical professional. Do not rely on the information on this Website as an alternative to medical advice from your doctor or other qualified professional healthcare professional or healthcare provider.
This is the module test for ‘HEARTe 11. Inherited and congenital cardiac disease’. It is strongly recommended that you work through the learning materials of the module prior to commencing this test. By going straight to the test you may miss out on valuable learning contained within the module. The answers to all the test questions are contained within the module. This information may have been provided in the ‘Additional Information’ boxes on some of the pages.
There are 10 questions and you must answer all of these correctly to obtain a certificate of completion.
You should allow approximately 10 minutes to complete the test.
Kirsten receives a 20 week scan which demonstrates that the baby is developing well, with no signs of congenital heart abnormality. She delivers the baby at full term in her local hospital. Kirsten will be reviewed by her cardiologist in the congenital clinic in four months time. This follow up will be life-long and will be shared between her local cardiologist and the specialist service for congenital heart disease.