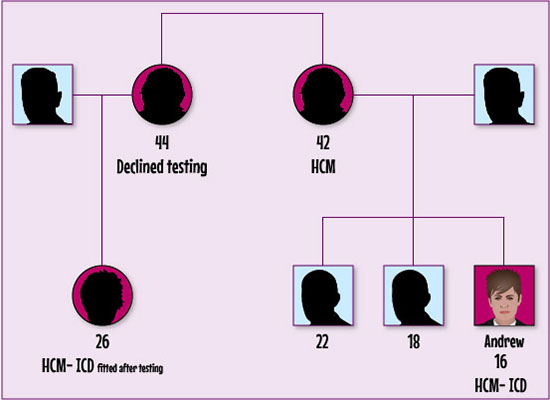
Following his referral to the cardiac genetic service, Andrew is offered a clinic appointment to discuss whether he would like to have genetic testing for the mutation that causes HCM. He and his parents decide that they would like to go ahead with this. Andrew is found to have the gene mutation and the family take the decision to offer other family members the opportunity to also be genetically tested.
In Andrew’s case, cascade screening of first degree relatives:
The main priorities with Andrew are to control any arrhythmias (his Loop recording showed episodes of non-sustained runs of ventricular tachycardia) and reduce the risk of sudden cardiac death. Management may involve:
- Optimal dosing with Beta-blockers (Bisoprolol). Beta-blockers improve ventricular relaxation and increase diastolic filling time. This should reduce the likelihood of ventricular arrhythmias occurring.
- Implantation of a subcutaneous Cardioverter Defibrillator (S-ICD). An ICD is a small device that uses electrical shocks or impulses to control potentially life-threatening arrythmias. Evidence suggests that S-ICDs have a number of benefits. They are easy to remove and replace, and require less extensive surgery than ICDs placed in the chest or abdomen. As there are no leads placed in the actual heart itself, the risk of infection in less. Patients should receive fewer unnecessary shocks as subcutaneous devices are more able to discriminate between normal and abnormal heart rhythms.
Andrew’s details are inserted into the European Society of Cardiology (ESC) HMC Risk-SCD Calculator
| Age (years): |
16 |
| Maximum LV wall thickness (mm): |
15 |
| Left atrial size (mm): |
35.5 |
| Max LVOT gradient (mmHg): |
30 |
| Family History of SCD (Yes/no): |
No |
| Non-sustained VT (Yes/no): |
Yes |
| Unexplained syncope (Yes/no): |
No |
The ESC HMC Risk-SCD Calculator recommends that Andrew should be considered for ICD implantation.
Please enable JavaScript in your browser to see this interactive content.
Following further discussion, at home, with his parents and family, Andrew decides to go ahead with the surgery to insert a sub-cutaneous ICD.
The GP suspects that Andrew’s presenting symptoms are suggestive of a cardiac condition and urgently refers him to the nearest cardiology clinic. Andrew attends the clinic, accompanied by his father, where he undergoes the following tests:
Please enable JavaScript in your browser to see this interactive content.
INTERACTIVE IS FULL OF LINKS
Based on the results of his investigations, Andrew is given a diagnosis of hypertrophic cardiomyopathy.
What is hypertrophic cardiomyopathy?
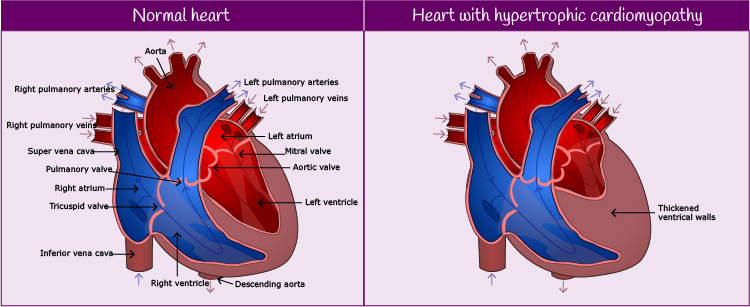
Hypertrophic cardiomyopathy occurs when the cells in heart muscle enlarge and cause the walls of the ventricle (normally the left ventricle) to thicken. It can be diagnosed at any age and is more common in men than in women. For more information on hypertrophic cardiomyopathy, please see Additional Information, below.

Meet Andrew

Andrew is a 16 year old school boy, who visits his GP complaining of frequent palpitations and dizziness while playing football.
He has had a normal childhood and adolescence,with no significant past medical history. He is not taking any medications.
Until recently, Andrew has undertaken regular sport, with no limitations, and played football for his school team.
There is no family history of unexplained collapses or sudden unexpected death.

A follow-up appointment is arranged for Margaret at her local Inherited Cardiac Conditions clinic and she will be invited to attend this clinic annually. Her daughter will also be invited to attend the cardiology clinic.
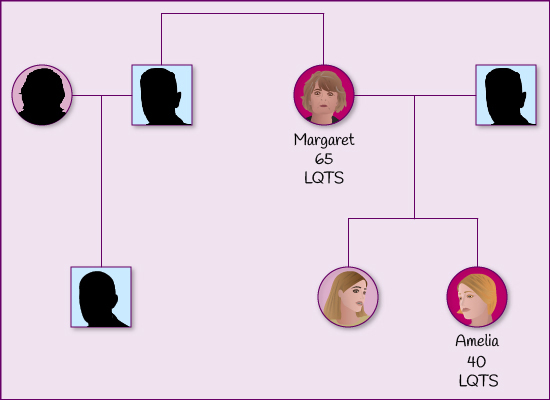
Although Margaret’s LQTS is drug induced, initial genetic screening finds that she has a gene pre-disposing her to LQTS. Margaret and her daughters are invited to attend the Inherited Cardiac Conditions Clinic for cascade screening. Those confirmed with LQTS will be offered annual revews at the clinic.
Genetic testing can raise a number of psychological, social and ethical issues for those individuals and families involved.
Please enable JavaScript in your browser to see this interactive content.
The genetic counsellor reassures Margaret and her daughters that she will be available to provide them with as much information as possible regarding any issues of concern.
One of her daughters has been found to have the LQTS gene mutation and is being referred to the Cardiology Clinic. Her other daughter has tested negative for any gene mutation.
Please enable JavaScript in your browser to see this interactive content.
What happens when Margaret is referred to the genetic clinic?
Please enable JavaScript in your browser to see this interactive content.
A management plan is discussed and drawn up with Margaret.
| Immediate |
Lifestyle |
Other considerations |
- Discontinue medications causing QT prolongation (Trimethoprim) & avoidance of QT prolonging drugs (www.crediblemeds.org)
- Start beta-blocker (Bisoprolol to Nadolol)
- Electrolytes (especially K
- Monitor for ongoing arrhythmia
|
- Long QT1 – avoid strenuous exercise and strenuous swimming
- Long QT2 – less adrenergically mediated, avoid exposure to loud noises
(There may be overlap within each long QT type so the general advice is applied to all)
- Diet – potassium rich foods encouraged and during periods of diarrhoea and vomiting electrolyte replacement is important
|
- Implantable cardiac defibrillator – if survivor or prior cardiac arrest without reversible cause (not appropriate for Margaret as her LQTS is reversible).
- Permanent Pacemaker for Long QT associated with bradycardia
- Testing of family members for LQTS
|
Margaret’s trimethoprin therapy is discontinued and she is commenced on a beta-blocker. After 7 days in hospital she is discharged home.
In order to confirm the suspected diagnosis of LQTS, Margaret undergoes a number of further investigations and tests. Whilst polymorphic ventricular tachycardia secondary to long QT may be drug induced, it is important, also, to investigate the possibility of underlying inherited LQTS.
Please enable JavaScript in your browser to see this interactive content.