What additional aspects of Sally’s management are important for the nurse to consider?
Category: HEARTe
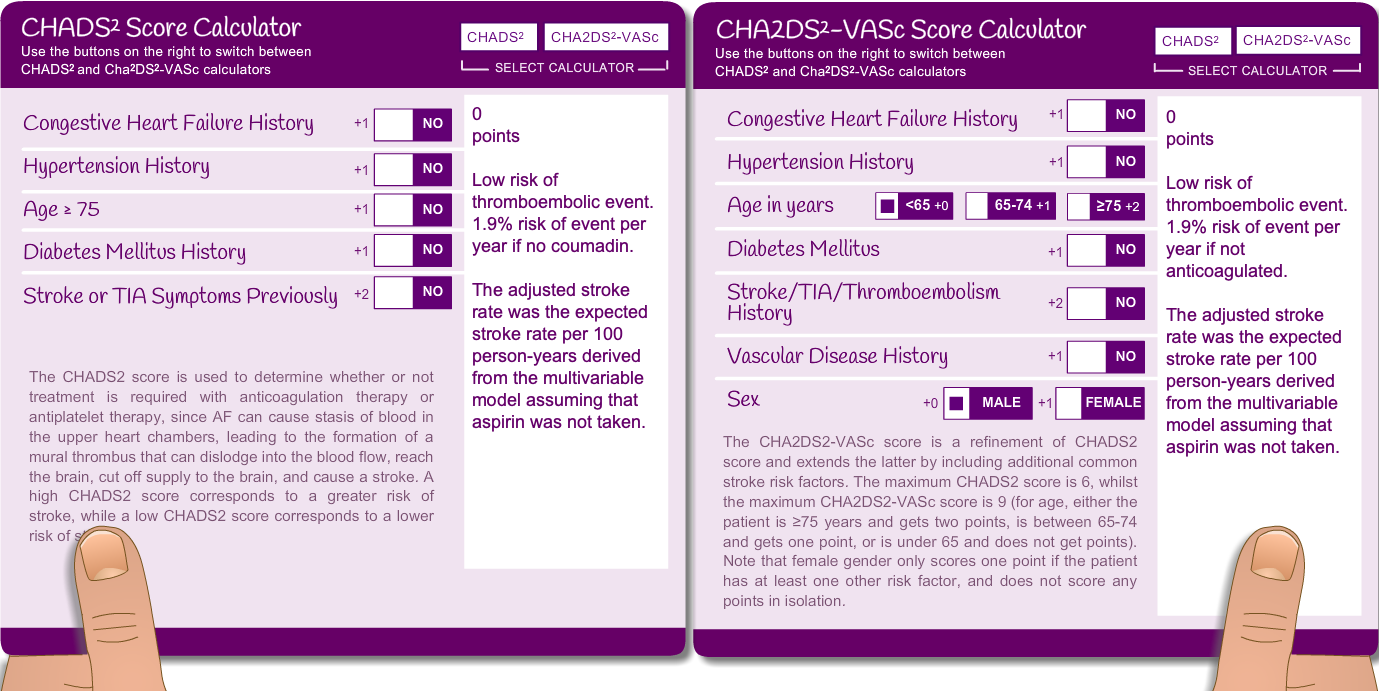
Sally’s results and stroke risk calculation
Sally’s 12-lead ECG shows AF rate of 120bpm. An echocardiogram revealed a dilated left atrium but is otherwise normal. Her blood results are all within normal limits.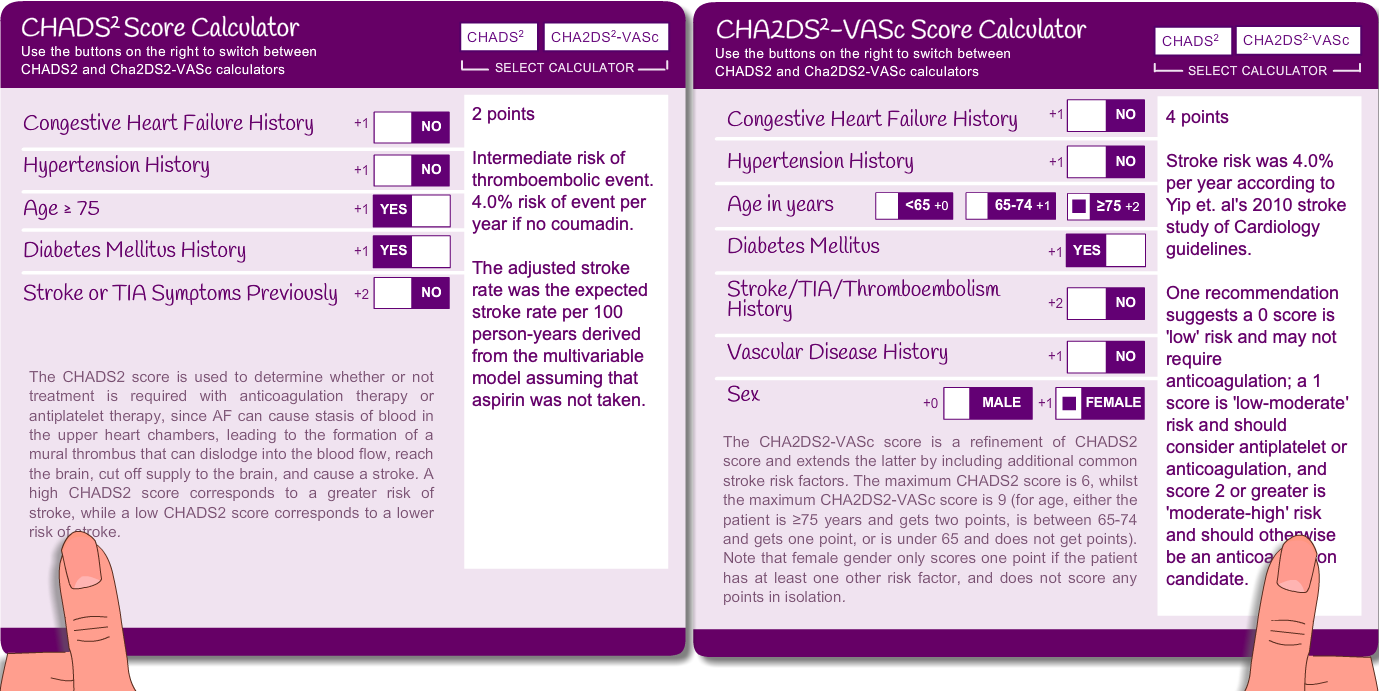
As a result of Sally’s high scores you would consider anticoagulation.
What next?
Sally attends the practice nurse
Case 2: Sally

Meet Sally
Sally is an 86-year old lady who has been experiencing shortness of breath when pottering around the house over the last few weeks.
She has type II diabetes which is well controlled with her diet. She lives by herself and her daughter lives near by. She doesn’t have any social service input, however her daughter does her weekly shopping and helps her with the hoovering.

Signposts
The GP’s summary notes
Having discussed the new diagnosis with Dillon, the GP writes up his notes.
Dillon’s stroke risk
Long-term management of AF
All patients should have their heart rate controlled to less than 110bpm at rest AND be asymptomatic of the AF.
This can be done either by “Rate” or “Rhythm” control, or sometimes a combination of both.
They both have advantages as well as disadvantages. As a result, the decision is made on an individual basis which is influenced by
- The patient’s symptoms
- Pre-existing cardiac disease/ other co-morbidities that predispose you to AF
- Length of time in AF (if the patient has no symptoms, this can be “guestimated” by the size of the left atrium. So if it is enlarged, they are more likely to have been in AF for a while).
- Size of LA: the more enlarged it is, the more likely someone is to stay in AF
- Medication options: based on lifestyle, potential side effects and other medical problems.
Rhythm Management:
This is when we try to return the patient from AF to sinus rhythm. This can be done either via DC cardio version or by using medications.
The most common medications used are: amiodarone, flecainide, dronedarone.
For patients who have symptomatic paroxysmal AF, are sometimes managed by a system called” Pill in the pocket”. This means that they take their rhythm control medication only when they are aware of the AF occurring, rather than taking it on a daily basis.
The British Heart Foundation have useful information about DC cardioversion.
Rate Management
This is the preferred choice for patients with longstanding AF and who have conditions that predispose them to AF. Rate control medications are probably safer than rhythm control medications.
The most common rate control drugs are: beta-blocker, rate-limiting-calcium-channel blocker, digoxin.
For patients who are aware of their AF (dyspnoea, fatigue, syncope and dizziness) it may be necessary to be a little more aggressive with the rate control (aim for a rate control of <80-bpm). People who have coronary heart disease may also require more aggressive heart rate control.
Consider causes and other issues
Dillon returns to the GP to be given his new diagnosis and management plan.
As part of Dillon’s holistic assessment, the GP explores and discusses the importance of Dillon self managing all relevant risk factors.