
Frank is now feeling much better, he’s managed to get himself a part-time job as a lollipop man. He is back attending his weekly darts games and Betty is glad he seems to be more like himself.
Frank knows more about living with his CRT-D and is more positive about life. He knows he will require to continue attending regular follow up and ongoing support. He is more aware of recognising any changes in his condition and feels he has more control in managing his long-term condition (learn more about self-management in long term conditions in the key themes module).
Frank has spoken to his employer and he can no longer drive a bus as he cannot hold a Passenger Carrying Vehicle (PCV) license with an ICD. Frank is worried about his loss of income and is concerned about how he will manage to pay his bills.
Click on the additional information box to see another illustration of Frank’s feelings in relation to living with his health condition.
For his follow up Frank attends the electrophysiology clinic. Patients who have had a CRT-D implanted require a clinical assessment and interrogation of the implantable cardioverter defibrillator (ICD). The nurse encourages Frank to consider his own priorities and set his own agenda. She gives him additional resources to enhance his understanding generally and also web addresses that he may want to access.
Frank leaves the clinic to talk things over with his wife.
When patients go home with a CRT /-D it is important that patients and family are given advice about living with the device.
In order to ensure that Frank is at the centre of all the choices in his future care, he should be supported and encouraged with self-management. Click on the following link to see Frank’s discharge letter (this is an example of what may be included).
Frank’s discharge letter [PDF]
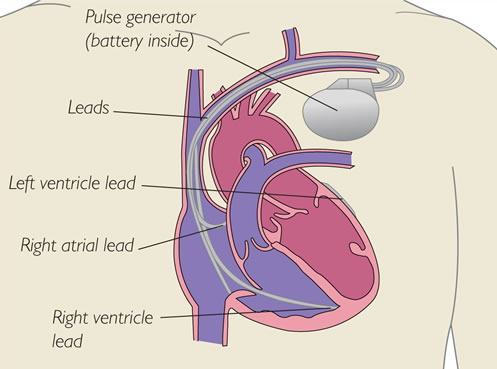
CRT is a pacemaker that has 3 leads which tries to coordinate the ventricles pumping action. The leads are placed:
- In right atrium
- In right ventricle
- Through coronary sinus and sits on outside of left ventricle
The battery is inserted under the skin on the left side of the chest. This procedure is performed under local anaesthetic and can take approximately 2-3 hours. There can be significant bruising post-insertion due to the insertion of the battery. Patients are advised not to lift their arm above shoulder height for the next 4-6 weeks until the leads are embedded in the hearts tissues.
Once the wires are embedded normal activities can be resumed but contact sports should be avoided.
As part of the procedure, many patients will also have a defibrillator integral to the device (CRT-D). In this case additional information is required. Patients are counselled about shocks and the device can be programmed to the individual needs. It is maintained with regular check-ups. Driving restrictions do apply depending on reason for implantation. Patients should be advised to check DVLA.
Patient and family/carer discussion using good communication techniques will be required when considering the options below in advanced care. The communication styles model within the key themes of HEARTe may help to clarify this and also the importance of considering self management within this scenario.
Remember a persons emotional reaction to their condition will clearly affect their motivation to pursue a self-management approach i.e. the social impact might be more crucial to address than the physical.
NB** Only when the QRS is prolonged and meets specific criteria, according to evidence based guidance and specialist review, is CRT a possible treatment option.
Once Frank is settled in to the Coronary Care Unit (CCU) the cardiologist comes to speak to Frank and Betty.
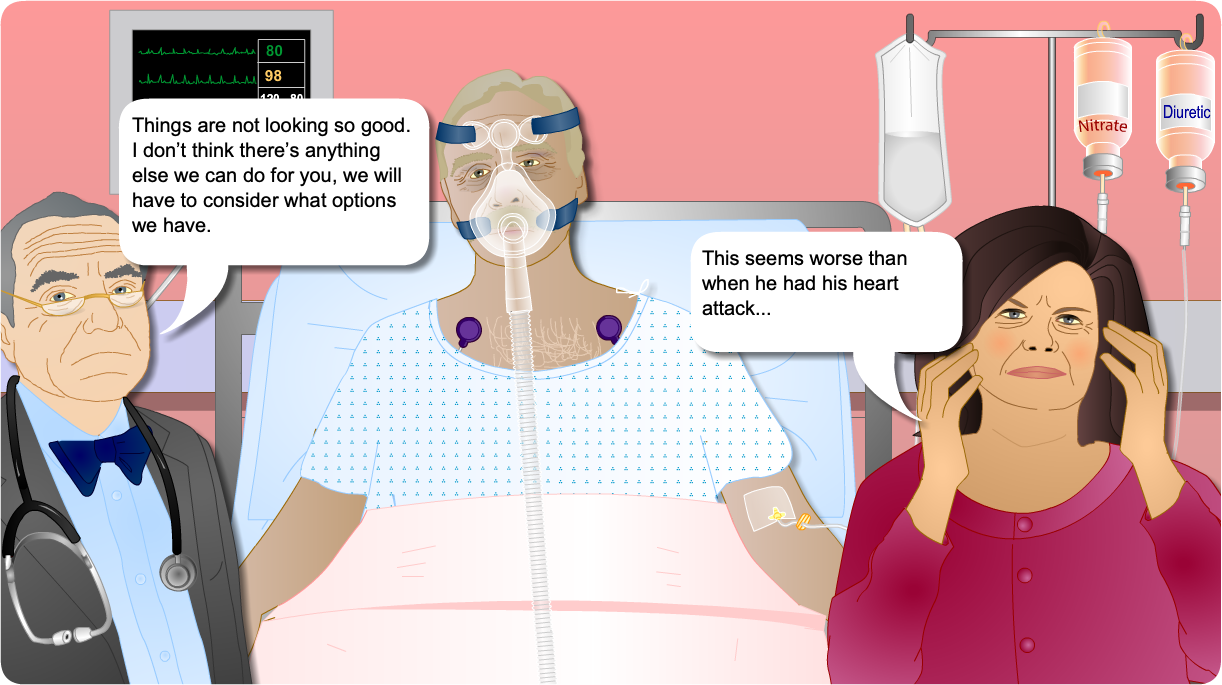
This isn’t the best way to break bad news, see the additional information box to find out what we should consider when breaking bad news.