Category: HEARTe
Consultation at RACP Clinic: taking a clinical history
Mary is referred to Rapid Access Chest Pain Clinic (RACPC)
RACPCs offer one-stop assessment clinic for patients who are experiencing new onset chest pain suggestive of stable angina, or increasing frequency or severity of symptoms of angina. The aim of such clinics is to quickly identify those patients at risk of an adverse cardiac event. Clinics are carried out by a specialist cardiology nurse or a member of the medical team who will determine/deliver appropriate tests to assist in diagnosis. In most cases an Exercise Tolerance Test (ETT) will be carried out in the clinic. This will normally take place in secondary care in a cardiology out patient setting.
There is no strong evidence to suggest that RACPC reduce admissions to hospital of patents with non-cardiac pain. However there is more positive evidence of earlier recognition of Acute Coronary Syndrome (ACS) and there is good evidence suggesting earlier specialist assessment leading to earlier diagnosis.
Let’s pause for thought
Consultation with the GP later that day
Annual diabetic review with practice nurse
Consultation at diabetic clinic
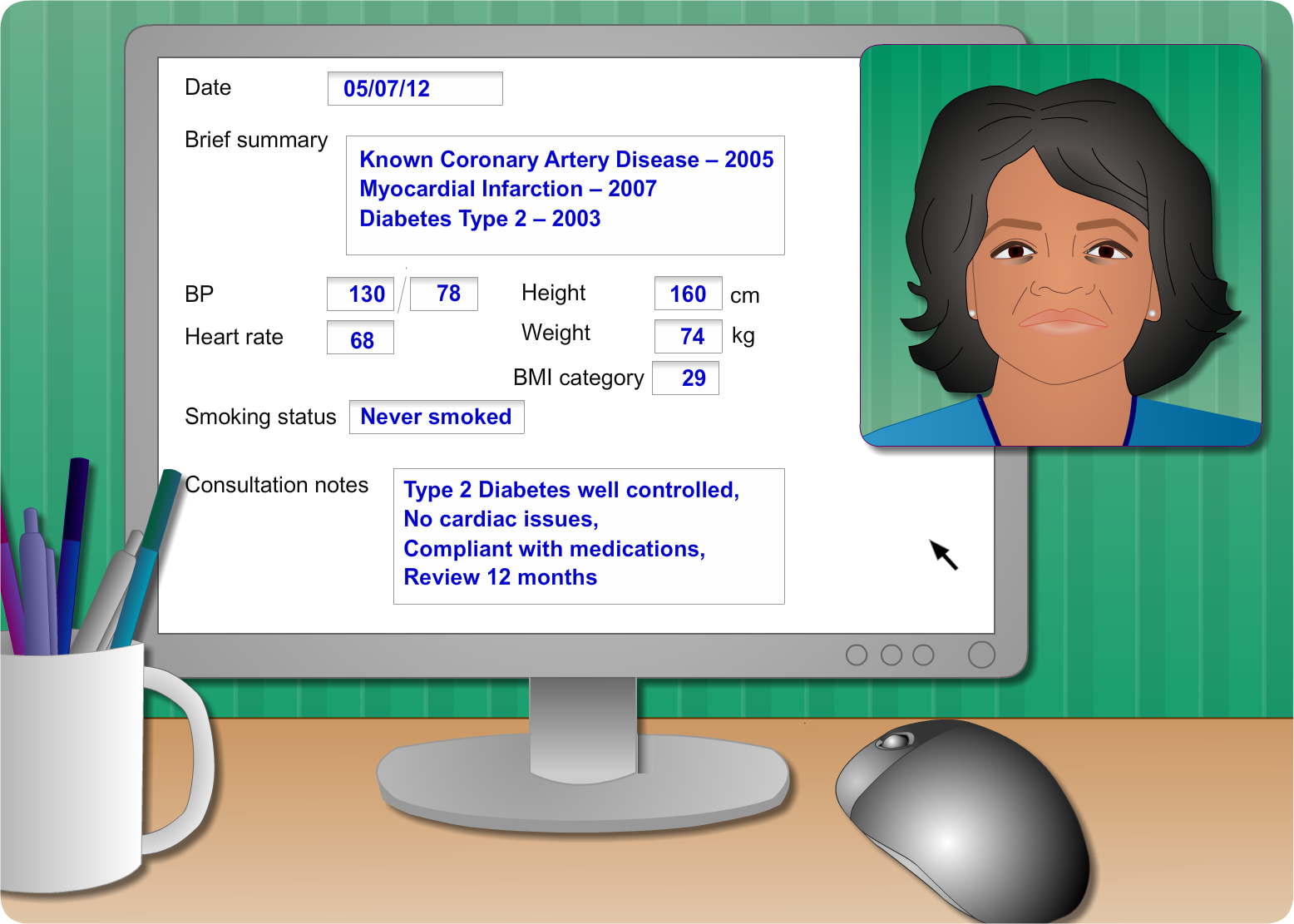
Mary attends the diabetic clinic for her annual diabetic review and the nurse takes her basic observations and looks at the previous consultation results.
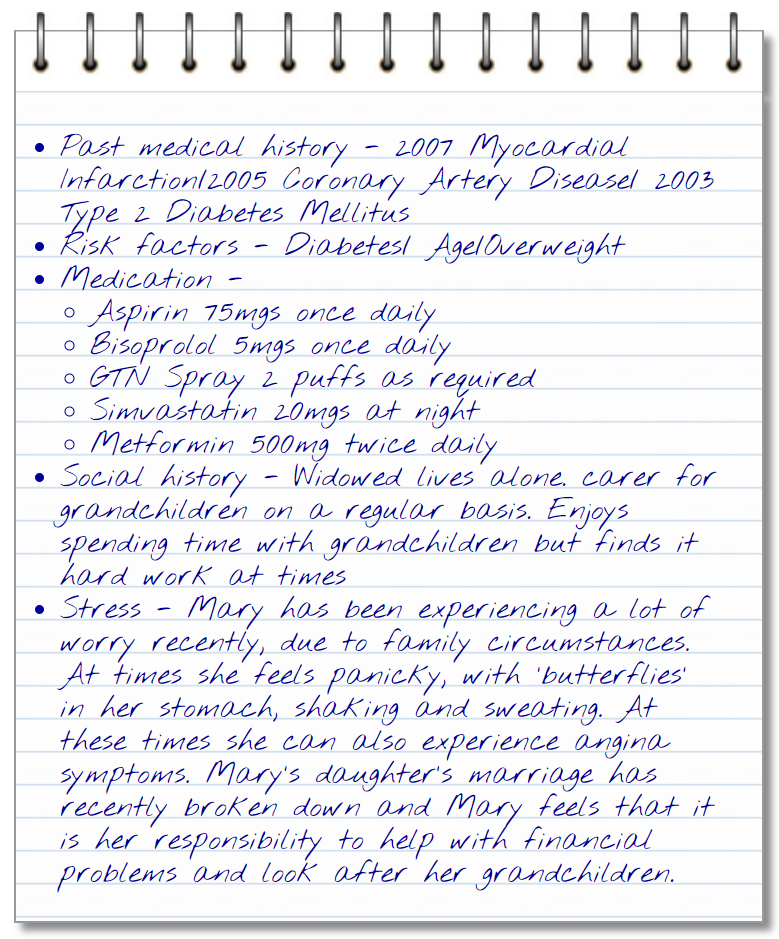
Mary is prescribed secondary prevention medications which she tells the nurse she takes regularly and hasn’t had any addition new problems with. (Aspirin 75mgs, Bisoprolol 5mgs, GTN Spray, Simvastatin 20mgs, Metformin 500mg twice daily.)
Mary


Mary is a 68-year old retired lady, who is a mother and grandmother. She is widowed, lives alone but is well supported by her family.
She enjoys cooking, sewing and a game of Bingo on a Thursday night.
Mary has type-2 diabetes and is well controlled with medication who attends her diabetic clinic once a year for a review at her GP surgery.
Key messages
The role of the healthcare professional is to:
- Take a good clinical history to aid diagnosis
- Ensure early assessment
- Recognise stable angina and risk stratify
- Commence evidence based treatment
- Explore the patient’s cardiac misconceptions
- Empower the patient to take responsibility for self management
To learn more about ETT preparation and the procedure please see Mary’s case or review Module 4.
Bryan’s new life
