Category: HEARTe
Bryan


Bryan may have misconceptions that he is doing sufficient activity but he is perhaps only watching sport.
Introduction to cases
Bryan is a 48-year old salesman who lives with his wife and three teenage children.
Mary is 68-year old retired widow. She is a mother and grandmother.
Ben is a 60-year old semi-retired civil engineer who enjoys a good lifestyle. He is a widow but has just met Senga.
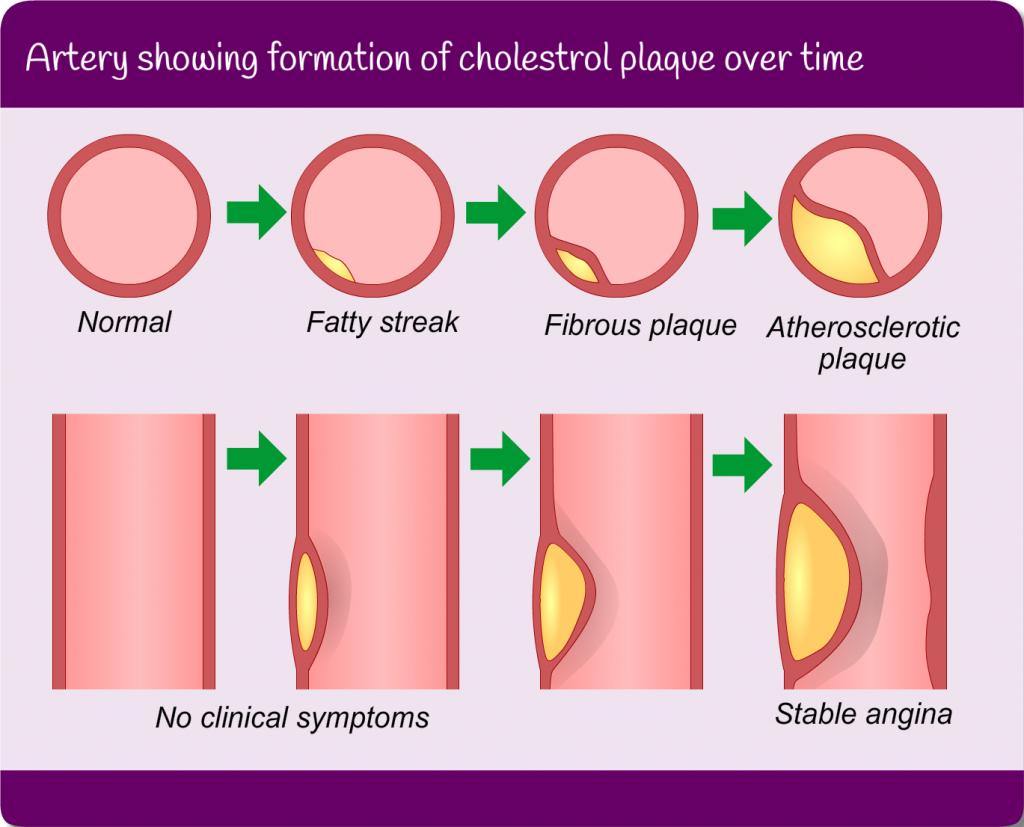
Atherosclerosis
Atherosclerosis is a potentially serious condition where arteries become furred up and narrowed by fatty deposits, including cholesterol. These substances are called plaques or atheromas.
The plaques cause affected arteries to harden and narrow. This is potentially dangerous for two reasons:
- restricted blood flow can damage organs and stop them functioning properly. This can affect many organs, including the heart (ACS/angina).
- if a plaque ruptures, it can cause a blood clot that blocks the blood supply to the heart, triggering a myocardial infarction (MI/heart attack) or to the brain, triggering a stroke.
Angina symptoms
Angina is pain or constricting discomfort (tightness) that typically occurs in the centre of the chest (but may radiate to the neck, shoulders, jaw or arms) and can be associated with breathlessness, nausea or sweating. It is normally brought on by conditions which temporarily increase myocardial oxygen demand e.g. physical exertion or exercise after eating or emotional stress or it may be brought on by exposure to cold, windy weather. It is usually predictable in onset and is normally relieved quickly by rest (less than 10 minutes) or by GTN spray.
It is important to be aware that the severity of the chest pain does not necessarily correlate with the seriousness of the underlying disease.
Reference: Braunwald, E. (1997). Cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. New England Journal of Medicine. 337: pp 1360-1369
Risk factors
Risk factors are conditions which affect your risk of developing cardiovascular disease. These risk factors can be “modifiable” – because they can be changed or treated, or “non-modifiable” – because you can do nothing to change them. You can learn more about risk factors in module 2.
Learning Outcomes
By the end of this module you should:
- Describe the pathophysiology of coronary artery disease
- Describe and define stable angina including signs & symptoms the patient may present with
- Demonstrate knowledge of targeted risk factor management
- Outline the pharmacological management of stable coronary artery disease
- Demonstrate knowledge of appropriate investigations and interventions for stable coronary artery disease (angina)
Epidemiology and discussion
Coronary Artery Disease is a preventable disease which kills around 8,000 people in Scotland each year. The disease is caused when the heart’s blood vessels, the coronary arteries, become narrowed or blocked and cannot supply enough blood to the heart. This can cause angina or a heart attack.
The recorded prevalence of angina varies greatly across UK studies. The average GP will see, on average, four new cases of angina each year (SIGN 96 2007).
The Health Survey for England (2006) reported that around 8% of men and 3% of women aged between 55 and 64 years currently have or have had angina. The figures for men and women aged between 65 and 74 years are around 14% and 8% respectively. It is estimated that almost 2 million people in England currently have or have had angina.
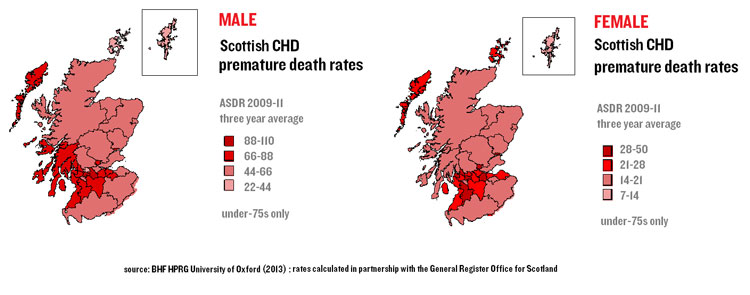
Scottish Government: Health of Scotland’s population – Mortality Rates
Coronary Artery Disease (CAD)
When the build up of atherosclerosis and atheroma affects the coronary arteries, it is called coronary artery disease (CAD) or coronary heart disease (CHD). When this affects the whole cardiovascular systems it is called cardiovascular disease (CVD).
Pathophysiology
When fatty deposits build up (arthrosclerosis) in the body the vessels become narrowed and there is a reduced amount of blood supplied to the cardiac muscle. This deposit is called atheroma.
Angina
Angina is the main symptom of myocardial ischaemia and is usually caused by atherosclerotic obstructive coronary artery disease restricting blood flow and, therefore, oxygen delivery to the heart muscle (NICE 2011).
Risk Factors
Risk factors refer to those factors which are likely to increase the risk of developing atherosclerosis and, therefore, CHD.
The image below shows stable encapsulated plaque, narrowing the lumen of the artery by approximately 50%.
Introduction

Module Authors
Module Lead
Frances Divers, Consultant Nurse, Lothian
Module Authors
Linda ONeill, Area Development Manager BHF, Scotland
Alpana Mair, Therapeutic Partnership Lead/ Prescribing Adviser, Scotland
Dr Katie Smith, Principal Clinical Pyschologist, Greater Glasgow and Clyde
Alison Keenan, Practice Nurse, Ayrshire & Arran
Reviewers
Katherine Paterson, Clinical Lead Cardiology Dietitian, Norwich University Hospital
Jane MacCaulay, Cardiac Specialist Nurse/Nurse Practitioner, Western Isles
Lyndsay Gentles, PN, Lothian
Susan Kennedy, NES Coordinator PN, Scotland
Louise Peardon, Deputy Director of Advice & Support, CHSS
Contributors
Brian Finlay, Community Resuscitation Development Officer (CRDO), Lothian
Louise Peardon, Deputy Director of Advice & Support, CHSS