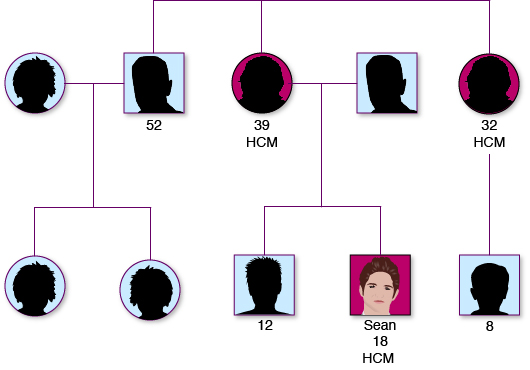
Unexpected cardiac arrest in the young is often due to undiagnosed hereditary conditions. Following investigations, Sean is found to be suffering from a hereditary condition known as hypertrophic cardiomyopathy (HCM).
Sean’s parents are, naturally, worried that their younger son may also have the condition and have an OHCA. They are visited on the hospital ward by a genetic counsellor. Genetic counselling is a process by which individuals at risk of a disorder that may be hereditary are informed of the consequences of that disorder, the probability of developing and transmitting it and the ways in which this may be prevented or lessened.
The aims of genetic counselling are to help the individual and family to:
understand the information about the genetic conditions
appreciate the inheritance pattern and risk of recurrence
understand the options available
make decisions appropriate to their personal and family situation
make the best possible adjustment to the disorder or risk
Genetic counselling allows information to be made available to “at risk” relatives, promoting early detection and treatment of inherited heart disease in these individuals. It affords the opportunity to address psychological/social/ethical issues which cannot be managed in a routine cardiology clinic.
Pulse point
Genetic counsellors are highly trained, registered healthcare professionals. Further information can be found at:
Following counselling, Sean and his family are referred to the cardiac genetic service and offered a clinic appointment to discuss whether they would like to have genetic testing for the mutation that causes Sean’s condition. Sean’s parents decide that they would like to go ahead with this, as they are concerned that his younger brother may also have the gene. Sean is found to have the gene mutation and the family take the decision to offer other family members the opportunity to also be genetically tested.
In Sean’s case, cascade screening of first degree relatives:
identifies inheritance from the maternal side, therefore, maternal relatives are offered screening
identifies asymptomatic gene carriers. These are individuals who are genotype positive (so have inherited the HCM gene) but phenotype negative (do not display the physical characteristics of the disease).
allows risk stratification for SCD to be undertaken and appropriate management offered to those of Sean’s relative deemed to be at risk.
(See Additional Information for best practice guidelines on genetic screening.)
A number of organisations offer support and advice to families in similar situations:
During Sean’s stay in hospital, his family visit regularly, despite living over 50 miles away.
Sean’s cardiac condition means that he requires to have an Implantable Cardioverter Defibrillator (ICD) fitted. Please see the video below for information on this:
Due to his head injury, Sean is unable to understand the implications of living with an ICD and for his parents the fact that they have to take responsibility for this aspect of Sean’s care is an added stressor.
Staff on the neurorehabilitation ward recognise that the family are finding their situation difficult to cope with and that they might benefit from additional support. They suggest to the family that a visit from the hospital chaplain might provide them with this additional support. They family readily agree and the chaplain is contacted.
The hospital chaplain provides spiritual support in the hospital environment to patients, family members and hospital staff. (For further information on spiritual care in the NHS, please see Additional Information below.)
Sean’s parents find the chaplain very supportive and, in addition to meeting as a family unit, meet on a one-to-one basis with him to talk over their worries and concerns in relation to Sean’s future.
Sean’s condition is critical and a decision is taken to dispatch an air ambulance to transport him to the nearest available intensive care bed. A helicopter arrives after another 20 minutes and delivers Sean to the nearest major hospital in just under an hour. Sean spends 48 hours in the intensive care unit. Although he is haemodynamically stable, Sean has acquired significant brain injuries.
The majority of those who survive an out of hospital cardiac arrest do not have significant neurological impairments. However, a small minority are left with severe brain injuries. This has major implications not only for the patient, but also for their family and loved ones. For information on brain injury following an OHCA, please see the following presentation by Lynne Atkinson, Edinburgh Headway:
Hypoxic/Anoxic Brain Injury
Hypoxic Brain Injury – reduced oxygen supply to the brain
Anoxic Brain Injury – interruption/no oxygen being supplied to the brain
The brain uses 20% of the oxygen you breathe. Nerve cells in the brain demand a high level of energy, thus after 4 minutes of reduced oxygen, brain cells will start to die.
The effects of hypoxic or anoxic brain injury can range from mild, short term symptoms such as reduced concentration and dizziness to longer term issues including speech and memory, dependant on the level of hypoxia experienced.
4 Main consequences of Brain Injuries
Physical
Cognitive
Executive
Psychosocial
Physical issues
Muscle weakness
Speaking difficulties
Tiredness/neural fatigue
Coordination/balance problems
Changes in sensation
Difficulty moving body parts in isolation
Neuropathic pain
Cognitive issues
Disorientation to time, place & person
Memory difficulties
Attention problems
Information processing problems
Spatial and constructional problems
Language problems
Executive Issues
Goal setting
Planning
Organisation
Self initiation
Self evaluation and monitoring
Flexible problem solving
Cannot predict consequences
Cannot monitor, predict or conceptualise time or money
Psychosocial
Personality changes
Reduced tolerance to frustration
Irritability
Emotional lability
Inhibition/impulsivity problems
Mood and emotional changes
Relationship difficulties
Reduced awareness/insight
Loss of motivation
Pragmatic disorder/dysfunction
The long term consequences are dependant on the severity of the anoxia and how much irreversible damage has occurred.
If there has only been mild anoxia, the person may make a recovery back to normal or near normal level of functioning.
For more information, please contact:
Edinburgh Headway Group
Headway House
Astley Ainslie Hospital
Canaan Lane
EDINBURGH
EH9 2HL
Following his resuscitation, Sean was hospitalised for several months and required intensive rehabilitation. Further useful information on brain injury and rehabilitation can be found at:
The team coach, Ewen, recognises that Sean has had a cardiac arrest and commences CPR. One of the by-standers phones 999. Bert, the local policeman, who is a trained Community First Responder is contacted by emergency services. He was out visiting in a nearby village when he was contacted and arrives with an AED 15 minutes after CPR has been commenced.
As was discussed in the Introductory section of the resource, the series of events required to resuscitate someone after an OHCA is known as the Chain of Survival.
Please enable JavaScript in your browser to see this interactive content.
Ewan, Bert and Sean’s family all feel very relieved that Sean’s care is now in the hands of healthcare professionals.
Sean Wright is an 18 year old teenager, who lives in a remote and rural village in the Scottish Highlands. (Please see Additional Information for Scottish Government’s Urban/Rural Classification.)
One Sunday morning, while playing for the village under-21 shinty team, Sean suddenly collapses. He has no medical history of note and did not appear to feel unwell prior to his collapse. His parents and his younger brother attend all his matches and are standing watching the game.
Once Edward was discharged from hospital, he felt that he wanted to contact the person who administered CPR and saved his life. Fiona recognised that she had not thanked Craig and wanted an opportunity to do so. They contact the store manager, who, having gained Craig’s permission, is able to provide them with his details. The couple visit the store and present Craig with champagne and chocolates, as a token of their appreciation.
Three days later after Edward’s OHCA, Craig’s manager invites him to come to her office for a debrief. Craig has been thinking a lot about what happened and welcomes the opportunity to talk to somebody about it.
Formal debriefing is a structured, voluntary discussion which aims to help individuals put what is, for them, an abnormal event, into perspective. Talking through the experience can help people clarify what happened and help them accept what has taken place. Not everybody will want to debrief and it should be an individual’s choice whether they participate or not.
Once they have transferred Edward to the Accident & Emergency Department, the ambulance crew are dispatched straight out on another emergency call. Alistair would have liked an opportunity to talk through what happened at the OHCA with his qualified mentor but there was no opportunity for this.
Instead, Alistair uses the event when he is asked to reflect on a critical incident as part of his clinical learning portfolio, using a structured model of reflection.
Please enable JavaScript in your browser to see this interactive content.
Peer support has been recognised as being hugely beneficial for those who have survived out of hospital cardiac arrest.
A number of regional cardiac peer support groups are available in Scotland. Information on these can be obtained from the Chest Heart & Stroke Advice Line Nurses:
Life After Cardiac Arrest – although an American site, this online support group contains a great deal of information for cardiac arrest survivors; the family/significant others of survivors; and responders:
Edward is an architect and owns his own practice, employing ten other people. He is keen to return to work as soon as possible following his discharge. A large percentage of those who survive an OHCA for 30 days or more return to employment.
Working Health Services Scotland provides free and confidential advice and health support for the self employed and those working in small companies.
Edward and Fiona live a few miles out of the city and are dependent on their cars for transport. Although Fiona is happy to drive Edward while he recovers, he is keen to be independent before he returns to work, as he often has to travel on site visits as part of his job.
General advice on driving after a cardiac arrest can be found at:
Life, motor and travel insurance can all be affected by the fact that someone has had an OHCA. The web sites below offer information on insurance companies who may be sympathetic to survivors but these frequently change. Edward found doing a search on a website that compared rates very helpful in finding the most preferential rates.
Following Edward’s cardiac arrest, Fiona notices that he doesn’t seem his usual self. She worries that the psychological impact of having had a cardiac arrest is having a greater impact on Edward than he has acknowledged.
Psychological reactions
Described below are some common psychological reactions following an cardiac arrest
Numbness
People described feeling ‘detached’ and the event may seem unreal, like a dream, something that has not really happened. Only in time may this numbness give away to feeling things more intensely.
Fear
Of having another cardiac arrest.
Of “breaking down” or “losing control”.
Of being left alone or having to leave loved ones.
Helplessness
Feeling of being powerless.
Sadness and grief
For loss of being healthy.
For loss of sense of being invulnerable.
For any life changes (e.g. giving up a job or hobby).
Guilt
For being better off than others, for having survived.
For having people worry.
Regrets for things not done.
Shame/embarrassed
For having been exposed as helpless, “emotional” or needing others’ help.
Anger
At what has happened.
At the unfairness and senselessness of it all.
At any shame or indignities suffered.
At other people not understanding or being inefficient.
Shock
Feelings of disbelief.
Questioning “why me?”
Need for privacy
Preference to be alone.
Relationship change
Shift in being carer/breadwinner to “being wrapped in cotton wool.”
It is estimated that around a fourth of individuals who have had an OHCA will show signs of anxiety and depression six months post-event.
A number of useful resources are available to help patients self manage their mental health and wellbeing:
Another strategy Edward learns about at his class is Mindfulness. Mindfulness is a simple, easily learnt approach to relaxing and taking time out from stress or worries. It is an adaptable and very safe skill that can be used as part of normal life. It is safe and effective in managing stress and worry. It has been shown to help with sleeping difficulties and generally helping people feel less driven.
Please watch the video below on mindfulness. Although the video was made for people who had suffered from a stroke, the content offers a good introduction to mindfulness and is equally applicable to individuals with a cardiac condition.
Chest Heart & Stroke Scotland: Being Mindful
Edward and Fiona both decide to use relaxation techniques and mindfulness to help them with cope with the impact of Edward’s OHCA.
Edward’s recovery is such that he does not require long-term support from Fiona to carry out his daily activities. However, this is not always the case with OHCA survivors and some family members may find themselves taking on the role of unpaid carer. There are a number of useful websites specifically aimed at supporting carers: