The NHS Scotland videos below show best practice applying orthoses. Click through the presentation carousel to view the different types of treatment in action.
Category: Advancing Modules
Side effects of antiplatelet agents
Prescription of anti-platelet agents
Benefits of aspirin (continued)
Benefits of aspirin
Benefits of aspirin for 100 stroke / TIA patients
- Without aspirin 25 patients might have a stroke during 1st year after a TIA or ischaemic stroke
- With aspirin only 20 might have a stroke (i.e. a 20% relative risk reduction – 25-20/25 x100% = 20%)
- Of the 25 who would have had a stroke, 5 avoid a stroke due to taking aspirin
- 80 did not have a stroke
- Treat 100 patients for a year and benefit 5
- Treat 20 patients for a year with aspirin and prevent one of them having a stroke (i.e. number needed to treat = 20)
- Each patient has a 1 in 20 chance of benefit from taking aspirin for the year
Choices of antiplatelets
Initial treatment in acute stroke: Aspirin is the recommended treatment and should be initiated as soon as possible and within 24 hours of symptom onset. Intracerebral haemorrhage should be excluded before commencing antiplatelets in patients with persisting stroke symptoms. Those intolerant of aspirin, despite the addition of a proton pump inhibitor, should receive an alternative antiplatelet medication. For patients with a minor stroke dual antiplatelet (Aspirin + Clopidogrel) can be considered in the short term.
NB: Anticoagulants are not recommended as an alternative to antiplatelet drugs in acute ischaemic stroke in patients who are in sinus rhythm.
Long-term treatment: Clopidogrel is the recommended treatment to reduce the risk of further cardiovascular events (Secondary Prevention). Those intolerant of clopidogrel should receive an alternative antiplatelet medication or combination of antiplatelet medication.
The combination of aspirin and dipyridamole is more effective that aspirin alone in preventing recurrent strokes, but dipyridamole is poorly tolerated due to side-effects, which include headache and diarrhoea. Although aspirin and dipyridamole in combination used to be widely used for secondary prevention, clopidogrel by itself is as effective and is now the main antiplatelet agent used for stroke prevention.
More information on Secondary Prevention Medication following stroke is available from: National Clinical Guidelines for Stroke for the UK and Ireland (2023).
Antiplatelet therapy
Introduction
Please note that this Topic Loop is under review and will be updated shortly to reflect the latest National Stroke Guidelines for Stroke (RCP 2023)
Antiplatelet medications, either singly or in combinations, are frequently used to reduce the risk of a further stroke after an ischaemic stroke or TIA.
- Antiplatelet agents make platelets less sticky and thus reduce clot formation
- Commonly used antiplatelet medications include: aspirin and clopidogrel
- The combination of aspirin and clopidogrel is not recommended for long term use after stroke because of an increased bleeding risk.
- Antiplatelet drugs increase the risk of bleeding – they should be used with caution in patients with a history of bleeding or anaemia.
- Other antiplatelet medication is available e.g. dipyridamole, prasugrel, ticagrelor but are not used routinely. This may change depending on new evidence.
More about anticoagulants
- Anti-coagulation should be considered for all patients in atrial fibrillation who have had an ischaemic stroke if no contraindication
- Warfarin is complex to use because its effects on clotting need to be monitored closely
- Warfarin can been effectively reversed during haemorrhage in less than half an hour using clotting products, e.g. Phytomenadione (Vitamin K), Dried Prothrombin Complex or Fresh Frozen Plasma (FFP)
- Warfarin has been shown to be the leading drug cause of admission to hospital for iatrogenic (caused by doctor) effects
- Warfarin has significant interactions with other drugs used in hospital resulting in significantly increased anticoagulation eg. amiodarone, ciprofloxacin, erythromycin and statins
- Specific antidotes exist for some of the DOACS if urgent reversal is required
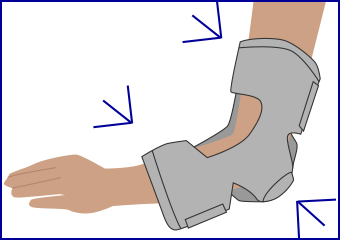
Elbow and hand orthoses
Elbow range of motion orthoses
Wrist Hand Orthoses (WHOs)
