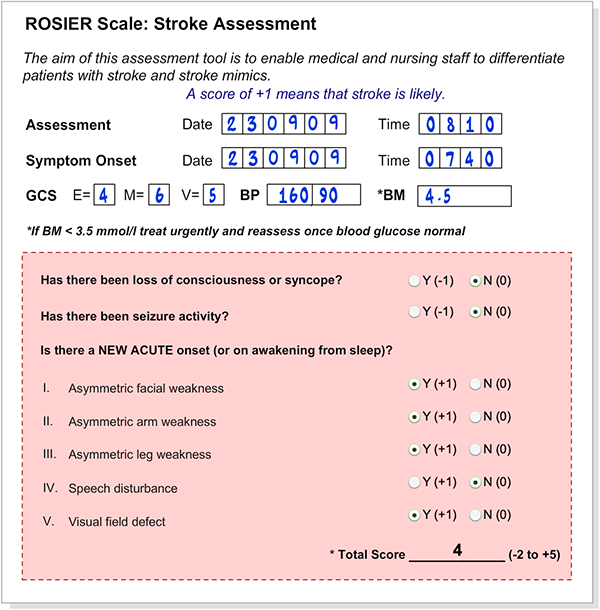
The ambulance arrived in A&E with Angela at 8.10am (30 minutes from onset). Her partner drove to the hospital to be with her. On examination Angela had no speech defects and was found to have a right sided facial and upper and lower limb weakness and right homonymous hemianopia. This would be detected by using the NIHSS scale. In some hospitals the Rosier score is used to determine how likely a diagnosis of stroke is.
Introducing the ROSIER scale
Duration: 1 min 05 sec
Using the ROSIER scale
Duration: 3 mins 00 sec
Here is Angela’s Rosier score
The A&E team now contact the stroke team to notify them of Angela’s admission.
Angela Campbell is a 65 year old lady. She lives with her partner, and was previously healthy and well. At 7am she got up and had breakfast.
At 7.30am Angela went for her morning shower. 10 minutes later her partner heard a noise and on investigation found Angela on the floor outside the shower wrapped in a towel. Realising that something was seriously wrong she immediately dialled 999.
Inclusive communication means sharing information in a way that helps everyone understand
For staff working in stroke services, it means recognising that people with communication difficulty understand and express themselves in different ways and therefore they need to find out what support is required and match the way they communicate to the ways the person will understand
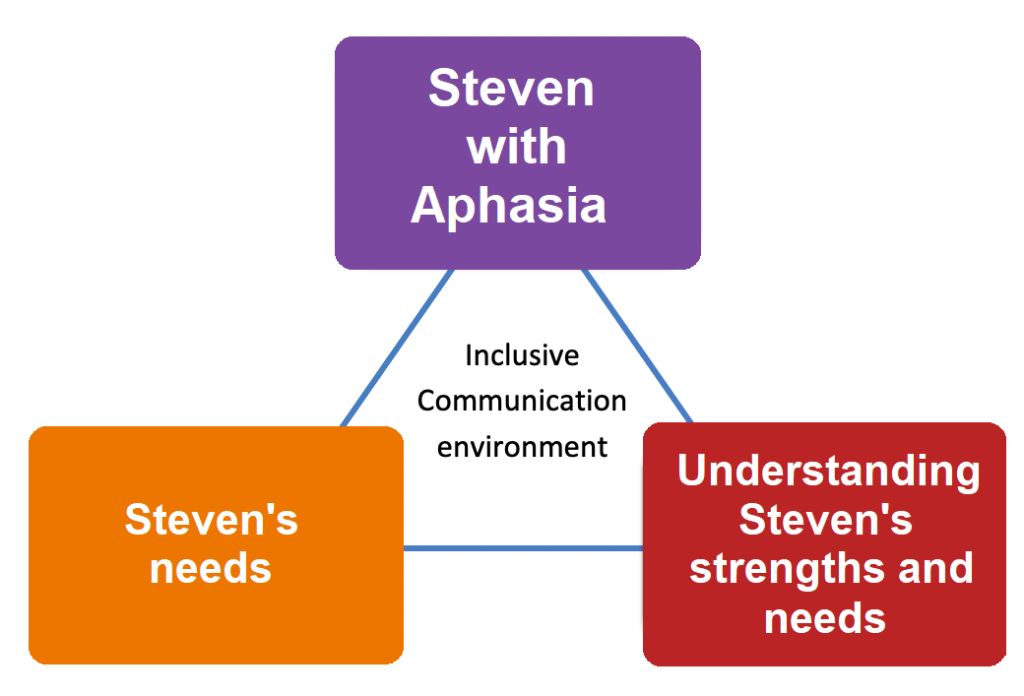
Due to aphasia, Steven will need supported communication to express his thoughts and feelings and without this is at risk of being misjudged in terms of his cognition and capacity. Click on link to training video Aphasia- what a difference some help makes.
RCP National clinical guideline for stroke 2016 states: “The carers and family of a person with communication problems after stroke, and health and social care staff, should receive information and training from a speech and language therapist which should enable communication partners to optimise engagement in rehabilitation, and promote autonomy and social participation.”
The ward aims to be an inclusive communication environment for Steven.
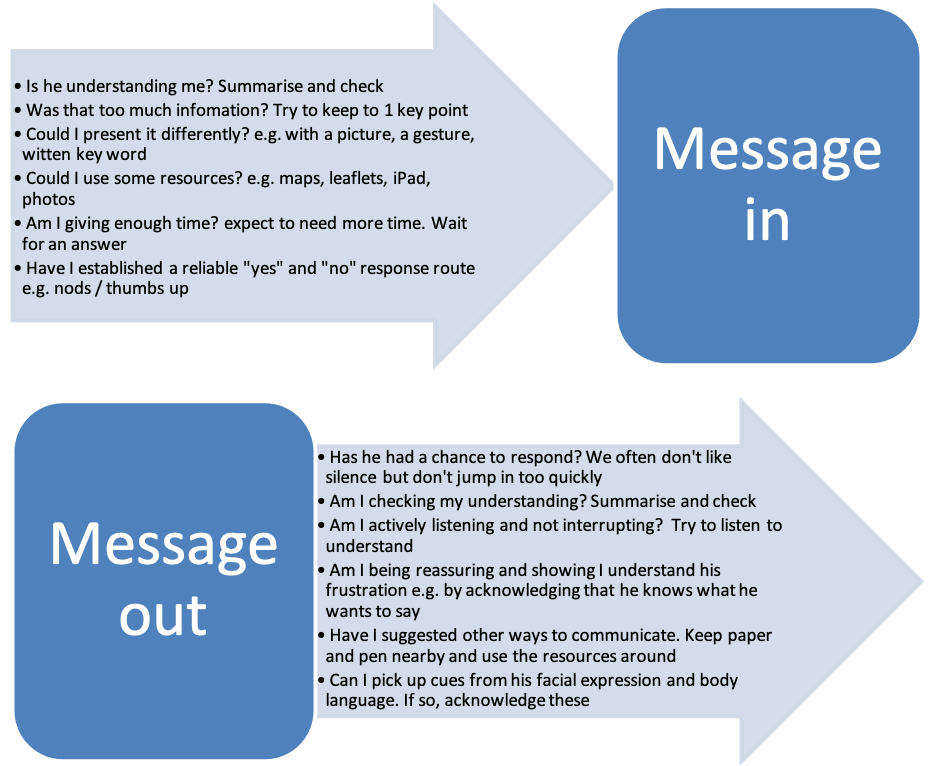
To be an effective communication partner with Steven requires some problem solving and thinking about how to adapt to make communication easier.
Keith normally keeps well, but has diabetes and was diagnosed with AF, and was put on an oral anticoagulant 3 months ago. He has been a little confused over the last month. He seemed OK when having breakfast at 8.00am, but his wife heard him fall at 8.30. She found he was unable to speak, had right facial droop weakness of his right arm and leg. He had hit his head and was bleeding from his nose. She called 999, the paramedics did the FAST test, they checked his BM which as 3.2mmol/l, pre-alerted the hospital and he arrived at 9.15am. His blood pressure was 210/90 when he arrived in the Emergency Dept.
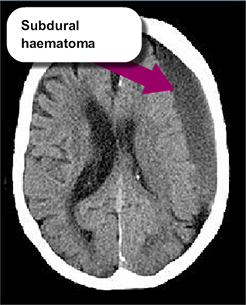
Keith’s CT scan
The CT scan shows a large hypodense (darker grey than brain tissue) subdural haematoma over the left hemisphere which is causing marked shift of the midline structures to the right and has effaced (i.e. squashed) the left lateral ventricle. The low density of the subdural collection suggests that it is chronic (i.e. has been present for some weeks). If the bleeding had occurred in the last few hours or days it would have appeared hyperdense (whiter than brain tissue, see CT 5 on the previous page).
In retrospect it seems most likely that the subdural has been present for over a month, was caused by the anticoagulation and caused his confusion over the last month. Subdurals can cause sudden worsening of neurological function mimicking a stroke.
Should Keith be treated with thrombolysis or thrombectomy? Select Yes or No. Explore the slides for more.
Keith Hughes-Smith is a retired 78 year old married man.
His story
Keith normally keeps well, but has diabetes and was diagnosed with AF, and was put on an oral anticoagulant (Apixaban) 3 months ago. He has been a little confused over the last month. He seemed OK when having breakfast at 8.00am, but his wife heard him fall at 8.30. She found he was unable to speak, had right facial droop and weakness of his right arm and leg. He had hit his head and was bleeding from his nose. She called 999, the paramedics did the FAST test, they checked his BM which as 3.2mmol/l, pre-alerted the hospital and he arrived at 9.15am. His blood pressure was 210/90 when he arrived in the Emergency Dept.
Which symptoms make stroke, more or less likely and which increase the risks of thrombolysis?