Q. Alice’s main goal is to walk, however the team agree this is unlikely. What should you do now? Select true or false for each of the options listed below.
Following your discussion with Alice she tells you exactly what she sees are the difficulties she experiences in relation to her walking and how she feels she can overcome them
Alice: ‘Okay, I know I struggle to get up from a chair and I need help, so I suppose I need to be able to do that to walk, and when walking in the gym the physios move my leg and stop me from falling. So that makes the physio’s think I can’t walk by myself. But I really think if I had a higher chair I could get up by myself and if they let me try a frame or a stick I would be able to walk without any help’
You now need to start writing her next set of goals with her, what are you going to set and how do you write them?
You and Alice look at the goals and discuss the outcome. From the information gained from the MDT meeting what are the outcomes from Alice’s goals? Use the outcomes scoring key below to help you decide.
| Goal Outcome |
Definition |
| A = Achieved |
The patient has consistently completed all components of the goal. |
| P = Partially Achieved |
The patient has consistently achieved a recognisable component of the goal but not the whole task e.g. if the goal is to get up and walk with help of one and the patient has only achieved the sitting to standing component then the goal is only partially achieved. If a patient inconsistently manages a goal this does not count as a partially achieved goal. |
| E = Exceeded |
The patient has exceeded the goal set e.g. if the goal was to walk in the ward with supervision but the patient is now independently mobile then it would be documented that they had exceeded the goal set. |
| N = Not Achieved |
The patient has failed to consistently achieve any components of the goal set. |
Q. What are the outcomes of Alice’s current goals?
That afternoon the key worker meets with Alice to feedback from the MDT meeting and to review and discuss her goals.
Follow the conversation Alice has with her key worker. Go through the slides to move from scene to scene.
The multidisciplinary team (MDT) have gathered for their weekly MDT Meeting. The team have just begun discussing Mrs Alice Rowan.
Go through the slides to see the team members and find out how Alice is progressing.
At the MDT meeting it is agreed that the key worker will now go and meet with Alice to agree her goals.

Introduction
Mrs Alice Rowan is a 68 year old lady who collapsed by the swimming pool while at her holiday home in Lanzarote. She was admitted to the local hospital with complete loss of movement down her left side. Two weeks later she was flown back to the UK and admitted to her local stroke rehabilitation unit. She has had 3 months of intensive rehabilitation and in that time she has made some steady progress. However her physical ability has remained the same for the last 4 weeks and the team feel that she is unlikely to regain the ability to walk. Her husband who is fit and well is very keen to take her home to their bungalow with support as required.
Outcome

Alan left hospital after 6 weeks and returned home with ongoing rehabilitation. He is able to walk with his dog, Patch, and socialise with his brother and friends. He has also found it beneficial working through the Self Help4 Stroke self management resource recommended to him by his therapy team.
Key Messages
- Patients spend a limited time in therapy and therefore self practice in environments out with therapy should be supported and actively encouraged to maximise their outcome
- Various options are available in the management of spasticity and should be considered early on
- Orthotics, of any sort, that are provided should have a clear management strategy
- Physical therapy interventions should aim to address a patient’s needs and requirements in relation to their rehabilitation. Patient input is a vital part of the rehabilitation process. By listening to Alan’s concerns the rehabilitation team were able to formulate an effective treatment plan that met his personal goals.
To learn more about the management of tone and spasticity following stroke visit STARs AM 19: Management of Tone and Spasticity After Stroke: A Role for Everyone.
To learn more about self-management and the strategies which may be used in the process of self management visit STARs AM 15: Self Management.
Two weeks later Alan is walking independently around the ward area. He walks outside with supervision and a stick. He will be independent in another week and his discharge date has been set. He continues to require FES for his dropped foot although some increased activity in his ankle muscles has been noted and it is hoped that he will not require FES long term. The therapist has discussed with Alan organising bringing Patch into hospital so he can practice walking with his dog.
See additional information for links to resources on pet therapy in healthcare settings.
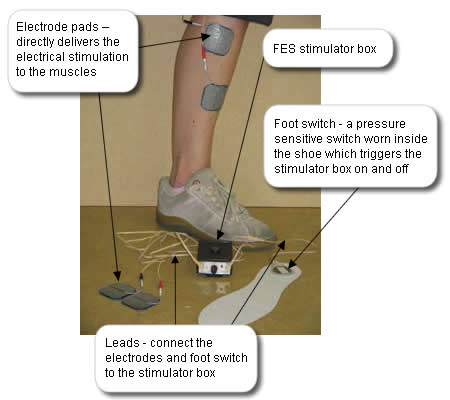
Alan’s physiotherapist is trained in the application of an alternative orthotic device for managing his dropped foot, Functional Electrical Stimulation (FES). She feels that this device may benefit Alan so she discusses it in detail with him, provides written information and gives him time to consider if he wishes to try it.
An FES Device
Watch the video below to see a stroke patient who presents with a dropped foot walking. Then watch the same gentleman walking but this time using an FES device to correct his dropped foot.
Duration: 1 minute 1 second (no audio)
The FES Device shown is Odstock Dropped Foot Stimulator (ODFS) from Odstock Medical Limited Salisbury. Other and newer FES devices are available .
Definition:
FES is a means of producing contractions in muscles paralysed due to central nervous system lesions (eg stroke) by means of electrical stimulation to the peripheral nerve (the nerves that are out with the brain and spinal cord). This stimulation is used to produce a functional movement e.g. lifting the affected foot during the swing phase of walking. Stimulation can be applied via surface-applied or implanted electrodes.
Impact of FES:
FES potentially has a therapeutic effect. This being the effect seen when the stimulator is switched off. By its mode of action, namely stimulating muscle, FES may encourage motor recovery.
Similarly to an AFO it also has an orthotic effect that being the effect seen while the stimulator is switched on.
Contraindications:
Exposed orthopaedic metal work on the lower limb; tumour in the area of stimulation; uncontrolled epilepsy; lower motor neurone conditions (conditions that have caused damage to the peripheral nerve)
Cautions:
Marked spasticity, poor skin condition; marked oedema (swelling); pregnancy; pacemakers; fixed ankle contracture
Rationale:
Alan meets the inclusion criteria for FES. Additionally, as Alan has some motor activity at his ankle it is considered that FES may help the motor recovery of his ankle and forefoot muscles. Following his discussion with the physiotherapist Alan is keen to try it and is therefore set up and provided with FES.
References:
| Ankle Foot Orthosis (AFO) |
| Why use it? |
An AFO can be used to assist with a patient’s walking. It can be used to directly control the dropped foot during the swing phase of walking. An AFO can also have an impact on the standing phase of walking by directly improving the stability and alignment of the ankle and foot on the ground which in turn may have an impact on the hip, knee and trunk position. |
| When to consider an AFO? |
As soon as the patient is medically stable consideration can be given to the provision of an AFO. |
| Cautions |
Poor skin condition, marked and fluctuating oedema (swelling), sensory loss, poor circulation, severe spasticity and marked contracture. |
| Rationale |
Alan has a dropped foot which causes his foot to catch when he swings his leg through during walking. Additionally when he stands on his leg his knee flicks back. The provision of a custom made AFO will help him swing his leg through during walking and indirectly reduce the flick of his knee into extension on standing. It is hoped that this will improve his gait pattern, independence and balance and reduce the effort of walking and potential for trauma to his knee joint. |
Reference: NHS Quality Improvement Scotland: Use of ankle-foot orthoses following stroke – Best Practice Statement